Understanding the limitations of integrated workcells

Overburdened and understaffed, today’s core labs are being asked to continually improve their performance under increasingly stringent operational constraints. Studies estimate that as many as 8,000 more laboratory technologist graduates are needed, per year, to keep pace with demand.1 Yet, despite this shrinking labor market, and having limited access to financial resources, labs are beset by requests from management to increase reliability, establish standardized procedures, and return results in less time – especially for STATs. Adding to this pressure is a steadily growing workload fueled by the increased healthcare consumption of an aging population.
These challenges notwithstanding, hospitals, in particular, are seeking ways to drive even more value from labs while decreasing their average costs per test. This steadfast commitment is mostly owing to the fact that labs typically consume three-to-five percent of hospital operating budgets. To meet these expectations, a growing number of hospital laboratories have begun investing in total laboratory automation solutions. The advantages of total lab automation are myriad; these systems minimize human errors, accelerate turnaround times, standardize processes, protect result integrity, and maximize the productivity of limited staff resources.
So why hasn’t every lab invested in a robust automation solution? The answer is simple. Most comprehensive laboratory automation solutions are too large and too expensive for the majority of today’s labs. So instead, many have begun investing in what they consider to be their only option for achieving automation-enabled performance improvement: integrated workcells. Crediting the analytical efficiency gained by connecting chemistry and immunoassay analyzers within a single frame, purveyors of integrated workcells promise to deliver meaningful performance improvement at an approachable size and price point.
In reality, however, integrated workcells alone are incapable of delivering the end-to-end workflow optimization that is required to significantly improve laboratory performance. Moreover – and, most importantly – integrated workcells leave laboratories unwittingly exposed to numerous risks that, when realized, drastically outweigh any benefits provided by analytical efficiency.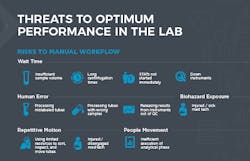
Productivity risks and increased costs
While touted as a solution designed to boost productivity, integrated workcells actually leave numerous productivity risks unmitigated across the laboratory workflow. Typically, a laboratory’s workflow comprises 32 manual steps, the majority of which are completed during the pre- and post-analytical phases. An astounding 80 percent of productivity risks occur during these phases, including insufficient sample volumes, long centrifugation times, delayed STAT start times, and mislabeled samples, among others.2 Integrated workcells, which contribute most of their value by streamlining portions of the analytical phase, do nothing to address these risks to productivity, leaving their laboratories fully exposed to the slower turnaround times and increased costs per test that inevitably result.
Protection from pre-analytical errors
Many of the risks that integrated workcells fail to address lead not only to diminished productivity, but also to diminished patient safety. An estimated 75 percent of result errors can be traced back to pre-analytical mistakes that were not caught prior to analysis. Despite that alarming statistic, today’s integrated workcells deliver no pre-analytical error evaluation.3 Instead, integrated workcells leave this important and arduous responsibility squarely within the jurisdiction of already-overloaded laboratory technologists. Given their long shifts and broad duties, and the inherent propensity for all humans to make mistakes, it is little wonder that, in this environment, many pre-analytical errors go unnoticed into the analytical phase.
Specifically, integrated workcells do little to help laboratorians identify mislabeled tubes, tubes containing wrong samples, or tubes carrying insufficient sample volumes. Such errors can put patients’ safety at risk, damage the credibility and reputation of labs, and expose hospitals to liability.
Importantly, these errors can also lead to the accrual of significant operational costs. Consider that a typical “medium-sized” hospital laboratory processes around 182,500 tubes per year.4 Studies show that approximately 0.66 percent of these tubes will come into the laboratory with one of the aforementioned errors, and that 72 percent of those tubes will directly contribute to additional costs.4,5 How much cost? On average, $208 per pre-analytical error in the U.S.5 Simply multiplying these factors together shows that, without enhanced help in identifying pre-analytical errors, a laboratory of this size can expect to incur approximately $180,000 per year in costs related to mislabeling, wrong samples, and insufficient sample volumes, alone.
Handling tubes and safety risks
Patient safety, hospital operating costs, and laboratory reputations are not the only things that integrated workcells do little to protect. Indeed, the safety of lab techs must also be included in this category. The reason is simple. Unlike with more-comprehensive automation systems, using integrated workcells alone means that lab staff must manually perform the majority of tasks in their lab’s pre- and post-analytical workflow phases. Of course, performing these tasks manually means that techs must personally handle tubes. And the more techs handle tubes, the more their health and safety are exposed to risk.
It should come as no surprise, then, that lab techs experience high incidences of repetitive stress injuries and infection as part of their jobs. In fact, the rate of Carpel Tunnel Syndrome (CTS) among techs hovers at around 10 percent.6 This trend is important because those suffering from CTS can be out of commission for weeks and even months as they undergo treatment and, if necessary, surgery and rehab. This not only negatively impacts quality of life for techs, it leads to lost productivity and higher costs for the labs that employ them.
With integrated workcells doing little to obviate the need for manual manipulation of tubes, techs who work in labs that have not adopted more comprehensive forms of automation can expect their risk of developing CTS and other stress injuries to remain undiminished. Furthermore, techs in such labs can expect little in the way of enhanced protection from being infected by e. coli, N. meningitis, Brucella, and other microbes and viruses.7 This is because an estimated 44 percent of manual workflow steps in the lab can directly expose techs to biohazards, and integrated workcells automate very few of those steps.8 The importance of protecting frontline healthcare workers from infection has perhaps never been more apparent than it is today, in the midst of the novel coronavirus. It is, therefore, critical for labs to realize that integrated workcells are of little use on this front, and that more comprehensive solutions – ones that automate manual steps across all three workflow phases – are needed to achieve the enhanced levels of laboratorian protection that are especially warranted in light of ongoing COVID-19 pandemic.
Mundane work affects productivity
Among the many benefits of comprehensive laboratory automation systems is that they automate mundane, manual tasks. When a lab uses just integrated workcells, however, its techs remain forced to spend hours accessioning, inspecting, decapping, transporting, and recapping tubes. Such repetitive, rote tasks can cause disengagement to proliferate within a precious and limited talent pool. And when techs become disengaged with their work, their productivity decreases, the frequency with which they make errors increases, and laboratory operating costs rise.
In fact, studies show that disengaged employees have 37 percent higher absenteeism and 18 percent lower productivity than their engaged counterparts.9 As a result, disengaged employees in a lab will, on average, cost that lab about 34 percent of their salaries annually. Over the course of a typical laboratory-equipment contract term, this translates to hundreds of thousands of dollars of costs incurred due to disengagement alone.6 Unlike with integrated workcells, one of the key advantages of investing in more comprehensive laboratory automation is that such systems take over many of the lab’s mundane, repetitive, and rote tasks, freeing technologists to do more of the skilled, rewarding work they love. This, in turn, increases their accuracy, productivity, and engagement.
Integrated workcells and workflow automation
Given the considerable risks to patient and tech safety, quality of results, lab productivity, and operational costs that are left unaddressed by integrated workcells, it’s logical, and likely imperative, to assert that they are not effective stand-ins for systems that automate the majority of manual steps across the pre-, intra-, and post-analytical workflow phases. By leaving tubes in the hands of techs throughout the majority of the laboratory workflow, integrated workcells simply fail to address the most pressing challenges faced by today’s labs. Labs must find, and invest in, more comprehensive solutions – systems that deliver the primary advantages of total-laboratory automation while accommodating budget and size constraints. Only with those solutions will labs enable themselves to consistently deliver measurably increased value for patients, employees, and hospitals.
Workflow-optimization technologies
Fortunately, the industry’s most innovative and workflow-savvy vendors understand the universal need for end-to-end process optimization and, in response, have begun offering products that can deliver real performance improvement to all laboratories. They are doing so by leveraging powerful, yet affordable, cloud-computing to make state-of-the-art clinical informatics available to labs of all sizes. They are also introducing “lean total laboratory automation” solutions to the marketplace – systems that go beyond the capabilities of integrated workcells while remaining at size- and price-points tenable for most labs.
Given the significant cost, quality, and performance pressures of today’s healthcare environment, comprehensive workflow-optimization tools like these are quickly migrating from the realm of “cutting-edge” to that of “absolutely essential.” With this in mind, any laboratory looking to maximize return on their next capital-equipment investment would do well to ensure their technical vendor of choice includes true, comprehensive workflow optimization at the core of its proposal.
References:
- American Society for Clinical Laboratory Science. Clinical laboratory personnel shortage. https://www.ascls.org/advocacy-issues/workforce.
- COLA’s Insights into the cost-effective laboratory (https://www.cola.org/insights-newsletters/2015/March/insights.pdf).
- A review of medical errors in laboratory diagnostics and where we are today. https://academic.oup.com/labmed/article/43/2/41/2505001
- J Clin Diagn ResNov; 7(11): 2491–2493. 2013| LabMedicine, 41, 89-92. 2010| Clinical Chemistry 53:7, 1338–1342. 2007| DOI 10.1515/cclm-2013-0597 Clin Chem Lab Med 20135.
- Green, Clinical Biochemistry 46 (2013) 1175–1179
- J Occup Health. 2017 Nov 20; 59(6): 513–520. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5721273/.
- Ellen Jo Baron and J. Michael Miller. Bacterial and fungal infections among diagnostic laboratory workers: evaluating the risks. Diagnostic Microbiology and Infectious Disease March 2008 60(3): 241-6.
- Beckman Coulter workflow analysis; 14 out of 32 manual steps.
- Gallup’s “State of the global workplace” Report, 2017.
About the Author

Anthony M. Barresi
Sr. Marketing Manager of Workflow and IT Solutions at Beckman Coulter.