Utilizing digital imaging to determine optimal incubation times for routine urine cultures

Urinary tract infections (UTIs) are among the most common of all bacterial infections1 occurring more often in women than in men, at a ratio of 8:1. Half of all women experience at least one UTI by the age of 35.2 Approximately 20 percent of women between the ages of 18 and 24 have a UTI annually3,4 with one in three experiencing a symptomatic UTI necessitating antibiotic treatment by age 24.2,5,6 UTIs are also a common reason for healthcare visits in the United States. These infections result in an estimated seven million office visits, one million emergency department visits, and over 100,000 hospitalizations at an associated annual cost of $1.6 billion.2,6,7 Therefore, it is not surprising that urine constitutes the most common type of specimen submitted to the microbiology lab for culture.
When treated promptly and properly, lower UTIs (infections of the bladder and urethra) rarely lead to complications. However, if left untreated, even an uncomplicated UTI can have serious consequences such as spread of the infection from the bladder to one or both kidneys. When bacteria infect the kidneys, they can cause damage that may permanently reduce kidney function. This can lead to kidney failure in people who already have kidney disease. Thus, the efficient detection of the causative agent of an UTI, along with the antimicrobial susceptibility testing of the pathogen, can be critical for patient care.
Digital imaging for reading of microbiology cultures can lead to expedited release of results while maximizing the efficient use of laboratory staff. The following study focused on utilizing digital imaging and artificial intelligence to determine the optimal time for urine culture incubation in order to accurately detect significant urinary pathogens.
Material and methods
The laboratory’s current protocol was to process all urine specimens on an automated processing instrumentation and read urine culture images taken with the system on both blood agar and MacConkey agar plates at two time frames: 14 hours of incubation, and again at 24 hours of incubation. Previous data showed that the 14-hour image read resulted in the ability to work up approximately 20 percent of the all clinically significant culture growth.
In order to determine the optimal time for reading urine cultures, images taken from 946 patient urine cultures were compared every two hours on both media types starting at 11/12 hours of incubation up to 23/24 hours. Results for each specimen were recorded indicating the presence or absence of growth. If growth was present, the colony count and type of colonies present was recorded.
Urine specimens collected during the fall and winter months of 2017 were included in the study. All urine cultures were analyzed by observing digital images taken with the full laboratory automation every two hours.
Results
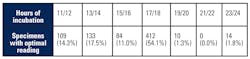
A total of 184 or 19.5 percent of the specimens were negative at each time frame images were read. Of the remaining 762 positive cultures, 109 (14.3 percent) had optimal growth at 11/12 hours of incubation, 133 (17.5 percent) after 13/14 hours, 84 (11 percent) after 15/16 hours, 412 (54.1 percent) after 17/18 hours, 10 (1.3percent) after 19/20 hours, and 14 (1.8 percent) after 23/24 hours of incubation. (Table 1)
A total of 242 (31.8 percent) of all positive urine cultures could have images read optimally at 14 hours of incubation, and 96.9 percent of all positive urine cultures had optimal image reading times at or before 18 hours of incubation. Twenty-four urine cultures (2.5 percent) showed optimal growth after 18 hours of incubation, however, 100 percent (24/24) of these cultures had growth detected on the blood agar on or before this time frame. Although they had not yet reached their optimal incubation time, these cultures would not have been called negative; they would continue to be incubated until such time that appropriate work up could be performed.
There was also a concern for possibly missing slower growing organisms after only 18 hours of incubation, such as yeast and alpha-hemolytic colonies, so these cultures were looked at individually. All cultures that contained yeast (25) or small alpha-hemolytic colonies (27) were also all detected as positive at or before 18 hours of incubation.
Discussion
Based on our patient population, changing our image reading times to 14 and 18 hours would allow for approximately 1/3 of positive urine cultures to be worked up after only 14 hours of incubation (including over half of the cultures that contained gram negative bacilli). The other approximately 2/3 of positive urine cultures could be worked up after 18 hours of incubation rather than needing to wait for a full 24 hours of incubation. In addition, the 3.1 percent of cultures that had optimal reading times after 18 hours of incubation would not have been missed as growth was detected for all of these at or before 18 hours; these cultures would continue to be incubated until they could be appropriately worked up. Likewise, the concern for possibly missing slower growing yeast and small alpha-hemolytic colonies after only 18 hours of incubation was mitigated as our data showed that all 52 cultures with these organisms were also detected positive within an 18-hour incubation period.
The data from this study indicate that the laboratory’s current 24-hour urine incubation time could be shortened to 18 hours using continuous incubation with digital reading without negatively impacting culture accuracy and reliability. In addition, we determined that the possible elimination of the first 14-hour image read would allow for streamlining the culture imaging process, reading cultures only once, and allow for more specimens to be accommodated by increasing our capacity. In our facility, instituting a single 18-hour image read would allow a more optimized work flow in the lab, effective utilization of microbiology staff, and have a positive impact to clinicians and patients delivering urine culture results hours sooner.
In summary
The final summary points from the study results are:
- Approximately 1/3 of positive urine cultures could be worked up after 14 hours of incubation (including over half of the cultures that contained gram negative bacilli).
- Approximately 97 percent of all positive urine cultures could be worked up after only 18 hours of incubation.
- Only three percent of cultures had an optimal reading time after 18 hours but they would not be missed as growth was detected at or before 18 hours of incubation.
- Instituting a single 18-hour read time for urine cultures would allow a more optimized work flow in our laboratory and have a positive impact on patients releasing urine culture results up to 6 hours earlier.
REFERENCES
- Nicolle LE. Epidemiology of urinary tract infections. Clin Microbiol Newsletter 2002; 24:135–40.
- Foxman B, Barlow R, D’Arcy H, et al. Urinary tract infection:self-reported incidence and associated costs. Ann Epidemiol 2000; 10:509–15.
- Hooton TM, Scholes D, Hughes JP, et al. A prospective study of risk factors for symptomatic urinary tract infection in young women. N Engl J Med 1996; 335:468–74.
- Brown PD, Freeman A, Foxman B. Prevalence and predictors oftrimethoprim-sulfamethoxazole resistance among uropathogenic Escherichia coli isolates in Michigan. Clin Infect Dis 2002; 34:1061–6.
- Rahn DD. Urinary tract infections: contemporary management. Urol Nurs. 2008;28:333–41.
- Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Am J Med. 2002;113:5–11S.
- Stamm WE, Hooton TM. Management of urinary tract infections in adults. N Engl J Med 1993; 329:1328-34.
Author acknowledgement: I would like to thank Copan Diagnostics for supporting our study.
About the Author

Cynthia C. Keyak, MT (ASCP), SSGB
serves as Microbiology Supervisor for Alverno Laboratories in Hammond, IN. She graduated from Purdue University with a B.S. in Biology, completed her ASCP Medical Technologist certification, and received her Six Sigma Green Belt from the University of Michigan at Ann Arbor. She is currently working towards her M.S. in Healthcare Administration.