How diagnostic stewardship is reshaping the modern lab

Three years after the pandemic, labs are at a pivotal point as they consider how to leverage their hard-won experiences and increased diagnostic capacity to build new standards for diagnostic excellence.
In my role on the Molecular and Scientific Affairs infectious disease team at Roche Diagnostics, I see labs across the country turning this pivot into a powerful opportunity to rethink their processes and ensure every test they run delivers the highest value to the patient. Two lab leaders from the University of Pennsylvania and Seattle Children’s Hospital recently shared how they have shaped their future by improving diagnostic stewardship and onboarding innovative solutions, such as flexible panel design and integrated clinical decision support tools, to improve patient care and lab efficiency.
At the pandemic’s end, Kyle Rodino, PhD, Assistant Director of the Hospital of the University of Pennsylvania Clinical Microbiology Lab and Director of the newly established Rittenhouse Molecular Infectious Disease Lab, and his colleagues were faced with the opportunity of a high-capacity lab that was no longer processing tens of thousands of COVID-19 tests per week.
“A silver lining of the pandemic is that the Rittenhouse Molecular Infectious Diseases Lab was born,” Rodino said. “It has equipment, personnel, and the associated infrastructure to do lots of different molecular testing, not just for SARS-CoV-2.” The opportunity was clear, but the puzzle remained: How do you harness this newfound capacity with diagnostic discipline to ensure that every test counts?
This new vision required close collaboration with many stakeholders to ensure the lab continued to serve the most common needs. One of the first actions was to audit lab send-outs, such as viral-load monitoring for HIV and transplant-related viruses and reclaim testing that could be performed internally.
“Now, you have the same viral load monitoring happening on the same platform by the same laboratory no matter where the patient enters the health system, so we get that longitudinal consistency,” Rodino said.
This centralization of infectious disease testing also freed up other departments to onboard more specialized diagnostics. For instance, the molecular pathology and microbiology teams were able to pursue adoption of new assays on their wish list.
“When we move testing out of a particular area [to Rittenhouse] that is more focused or aligned from a skills perspective with other areas of testing, they can backfill that now with innovative testing they’ve been wanting to do but maybe couldn’t previously because they were at capacity for testing volume and full-time employees,” Rodino shared.
Tackling overuse of testing
If onboarding new assays was the “what” of their evolution, diagnostic stewardship was the “how.” Early on, it was clear that real success also meant influencing clinical-ordering behaviors to ensure appropriate use of the available tools.
The team’s focus first turned to respiratory test ordering. A multidisciplinary Respiratory Pathogen Committee was convened to take a deep dive into institutional ordering practices. The committee’s first observation: A significant overuse of expanded respiratory panels was driving up costs without providing equivalent improvements in patient impact.
“The greatest benefit of the expansion of syndromic panels over the last decade has been access to all of these targets, but when you look at some of the panels, seasonality and patient populations, and when you apply them to different use cases, they don’t match perfectly,” said Rodino.
The team suspected that the increased ordering of these panels could be driven in part from heightened respiratory virus vigilance during the pandemic, but this was just part of the story. Now that the respiratory landscape had shifted, new guidance was needed.
The team sought to define a testing strategy rooted in appropriate test use. It referenced multiple resources, including Penn Medicine’s clinical ordering practices, guidance from the Association for Diagnostics & Laboratory Medicine (ADLM), and insurer medical-policy guidelines.
“We talked about the literature-supported use cases, but also uniqueness of Penn patients — such as how hematology–oncology was using testing for patients actively receiving therapy,” Rodino said. “Then we made a list of five indications that are ‘no-questions-asked’ indications for expanded panel ordering.”
Setting the standard was only the beginning. To achieve true stewardship, the lab had to move beyond the policy and into the clinic, finding the most effective levers to influence clinician behavior and align ordering habits with the new standards. The team considered many of the usual tactics, from provider education to EMR overhauls, and arrived at an integrated clinical decision-support tool that was implemented in September 2024 (see Figure 1).
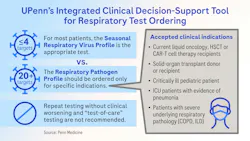
Now, when providers order an expanded respiratory panel within the EMR, they enter an ordering pathway with a note that explains the institution’s agreed upon use cases. The standard order is a seasonal panel with four or fewer targets whose identities change twice per year. Target selection is informed by regional prevalence and chosen by the Respiratory Pathogen Committee to provide the greatest diagnostic yield of the testing performed. To decrease duplicate testing, the tool also includes a list of results for all recently ordered respiratory testing for the patient.
Beyond the seasonal order, providers also have the option to select the expanded panel. For this selection, providers must specify the clinical need by selecting from a pre-defined menu of five indications. If the patient indication is not included on the list, the provider must provide a free-text description. Importantly, the presence of free text does not impede the diagnostic-ordering process, as the lab is not monitoring these on a case-by-case basis. Instead, the free-text descriptions are trended over time, and the feedback is used to identify opportunities for indication expansion and further tool optimization.
This integrated tool fundamentally shifted ordering habits within the first year. “What we’ve seen is a one-third decrease in the ordering of the large respiratory pathogen panel and a quarter or so of the people who entered the tool reroute themselves to the smaller panel,” Rodino said, noting that reagent spending also decreased by 30%.
Not all labs are the same
While every lab may face similar hurdles, the way they go about overcoming them depends on the needs of the populations they serve and the resources at hand.
Drew Bell, PhD, Director for Seattle Children’s Hospital’s Clinical Microbiology Lab, was similarly concerned with the post-pandemic overuse of expanded respiratory panels. He tackled this problem through collaboration with the Patient-Centered Laboratory Utilization Guidance Services (PLUGS), a “big engine of laboratory stewardship” within the Seattle Children’s system, Bell describes.
Bell and colleagues identified multiple unique drivers contributing to the increased ordering of expanded panels. Some of the increase was caused by an influx in pediatric admissions diverted from regional hospitals that had recently shuttered or lost their pediatric capacity. In these instances, the increase in test ordering was influenced by multiple external, and largely uncontrollable, factors, but was deemed appropriate for patient management.
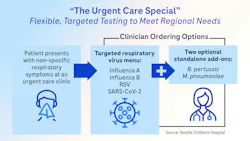
The team then turned its focus to the network’s urgent-care clinics. A deep dive into ordering practices at supported urgent care facilities identified that recent surges in Bordetella pertussis and Mycoplasma pneumoniae were primary drivers of expanded panel ordering. “Unfortunately, the way that our system had been built, the only way for our providers to get those answers was with the larger panel,” Bell shared. “If we had the standard flu/RSV/COVID test and the optionality to add on Bordetella or Mycoplasma, that would probably do away with most of the reasons that the larger panel was being ordered.”
In response, the lab established a standalone Bordetella pertussis assay and is actively working on developing a standalone Mycoplasma pneumoniae assay. Once all of these assays are available, the team envisions a future panel colloquially deemed “The Urgent-Care Special,” in which providers can easily request the standard viral four-plex assay with optional additions of the two bacterial targets (See Figure 2). “So if M. pneumoniae is having a bad year in the community, or there’s a Bordetella outbreak in the local public school system, you can collect one swab and run all three tests, no problem,” Bell stated.
Once these options are in place, Bell and team aim to remove the long respiratory panel from the available standard test menu for Seattle Children’s urgent-care facilities to curb unnecessary use.
As this news has circulated through their clinics, Bell said expanded panel usage has already gone down. This decrease is an indication of the influence that leadership can have on ordering behaviors. “You need to have your leadership on board,” Bell said. “If you change the system technically, that’s usually not enough to change human behavior. Your department leaders have to lead the change you want to see.”
The future is flexible
When asked about the future, Bell shared that flexibility is a must-have for panel design, optimally allowing for unique responses to constantly shifting pathogens and patient populations.
“The dream panel is always going to be changing depending on what is circulating, how much is circulating, and what the public health risks are at the time,” Bell said. “Also, patient populations change over time, and we want to be reflective of what our patients’ needs are.”
Rodino also believes that the future of diagnostic excellence relies on flexibility. “We would just be using all this testing power in a more responsible way,” he said. “We are approaching a phase two version of syndromic testing in which I would like to apply it in a more judicious manner to all of those different populations and instead of developing one-off LDTs to customize to the right population, testing environment, etc. I would like to use parts and pieces of the same panel where it is most appropriate.”
He sees flexible solutions as the catalyst for a new era of lab medicine, one that accelerates efficiency, transforms the patient journey, and sets a higher standard for care satisfaction.
In an era of rapidly shifting regional needs and evolving clinical complexities, the lab remains a primary driver of healthcare innovation. As we navigate the complex balance of diagnostic stewardship and innovation, decision-support tools and testing flexibility provide the power to respond to regional needs with precision. The path forward will never be predictable, or perfectly reproducible, but by learning from each other's breakthroughs, we can transform today’s challenges into a new standard of diagnostic excellence. Let’s lead the way, together.
About the Author

Alesia McKeown, PhD
is a Scientific Partner for Infectious Disease in Medical and Scientific Affairs at Roche Diagnostics. She is the subject matter expert for Roche’s high-throughput and POC respiratory solutions. She also co-leads an interdisciplinary team focused on improving access and utilization of diagnostics in the respiratory disease area.