Neonatal and pediatric drug testing: Reassessing adult-derived assay cutoffs

Neonatal and pediatric urine drug screening remains inconsistently standardized across institutions. Many laboratories apply assay urine drug screen (UDS) cutoffs derived from adult or workplace testing, despite key differences in newborn and pediatric physiology and specimens, including collection timing, dilution, and drug metabolite detectability.1 Adult derived thresholds may be too high and miss clinically relevant substance exposure in neonates and pediatric patients. Lower thresholds can improve drug detection but may also reduce false negative findings that may favor more definitive drug confirmations. Although some centers have adopted lower, locally validated pediatric cutoffs, a universal neonatal standard is lacking. Results should be interpreted in clinical context, and definitive or direct mass spectrometry confirmation should be obtained when findings may affect medical care or reporting drugs of misuse.1,5
Current testing strategies in neonatal and pediatric toxicology
UDS cutoffs developed for adults should not be used routinely in neonates because the newborn’s miniature body functions and practical collection issues can distort results.1,6 Neonatal urine is frequently diluted, the first void may be missed, newborn metabolism differs from adult metabolism, and intrapartum medications can yield misleading positives. When testing is warranted, cutoffs should be validated for neonatal and pediatric populations rather than adopted from workplace programs. Neonatal toxicology may be performed using urine, meconium, or umbilical cord tissue, and the choice of matrix affects the detection window.2 Urine generally reflects exposure in the hours to days before collection but can be difficult to obtain and is often diluted. Meconium and umbilical cord tissue largely capture third-trimester exposure; meconium can be more sensitive for certain drugs, whereas cord tissue is typically easier and faster to collect at delivery. Because discordant meconium and cord results are well described, findings should be interpreted cautiously and in clinical context.
Testing approaches vary by institution. Many laboratories screen neonatal and pediatric urines with an immunoassay and confirm only presumptive positive results by definitive mass spectrometry; presumptive negatives are typically not confirmed.2,5 Some pediatric centers bypass immunoassays and use direct liquid chromatography tandem mass spectrometry for selected pediatric patients, particularly when results may have significant clinical, legal, or child-protection implications or when broader analyte detection is needed. In perinatal and neonatal care, definitive or direct confirmation testing is especially important because false positive or false negative results can meaningfully affect management and family outcomes.
Understanding Tier 1 and Tier II drug testing
In this article, Tier I refers to rapid immunoassay screening such as enzyme multiplied immunoassay technique (EMIT) or enzyme linked immunosorbent assays (ELISA). Because these assays have short turnaround times, they are useful for initial assessment and emergency triage; however, results are not definitive and may miss clinically important exposures due to assay limitations. Tier-I EMIT/ELISA urine drug screen results are therefore presumptive.3 Presumptive positives should be interpreted cautiously and confirmed with Tier-II testing when results could affect clinical management, disposition, or referral to social services or child protection. Tier II refers to definitive confirmation of Tier-I findings by gas chromatography mass spectrometry or liquid chromatography tandem mass spectrometry (GC-MS or LC-MS/MS), which offer higher analytical specificity and sensitivity for detecting drugs of misuse. Tier-II can also include a direct LC-MS/MS testing confirmation without prior immunoassay screening (see Table 1).
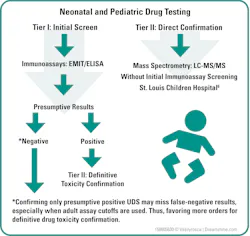
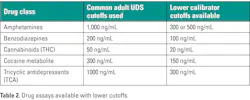
Qualitative and semiquantitative immunoassay Tier-I UDS remain widely used because they are practical, relatively inexpensive, and provide rapid screening in hospital laboratories, emergency departments, and point-of-care settings. Drug cutoff values are established according to the calibrator concentration used (see Table 2). Accordingly, neonatal and pediatric specimens may be validated and analyzed using lower cutoff thresholds than those applied to adult specimens.9 Many panels target amphetamines, benzodiazepines, barbiturates, cannabinoids (THC), cocaine metabolites, fentanyl, methadone, opiates, oxycodone, and tricyclic antidepressants. However, EMIT and ELISA assays can cross-react with structurally related compounds, producing false positive results. For instance, tricyclic antidepressant assays may cross-react with cyclobenzaprine or some antihistamines, and amphetamine assays may cross-react with drugs such as labetalol or venlafaxine. Conversely, limited assay sensitivity, high adult assay cutoff thresholds, or restricted drug menus can yield false negative results when clinically relevant drugs are present at low concentrations or outside the assay target profile in neonates and pediatric patients.4 Reducing the neonatal and pediatric UDS testing cutoffs in Tier I may result in decreasing false negative results, thereby favoring the definitive drug toxicity confirmation through mass spectrometry in Tier II.
Guidance from ADLM on clinically actionable drug testing
The Association for Diagnostics & Laboratory Medicine, (ADLM) guidance emphasizes that urine drug testing should be clinically actionable and interpreted with clear knowledge of test menus, sample types, assay cutoffs and limitations. Immunoassay results should be reported as presumptive or unconfirmed, with accessible cutoff information and interpretive comments addressing potential false positive and false negative findings. The guidance also recommends collaboration among laboratory professionals, clinicians, medical toxicologists, and poison control services to ensure that drug-testing menus reflect local drug-use patterns and patient-care needs. Although the document is focused on emergency care, its recommendations are relevant to neonatal and pediatric testing when results may affect clinical management, disposition, or downstream social and legal decisions.5
Evidence supporting LC-MS/MS testing in pediatric patients
St. Louis Children's Hospital assessed a one-step, broad spectrum LC-MS/MS method for drugs of misuse in pediatric patients, replacing the traditional immunoassay screen-and-confirm workflow.6 In the nursery cohort, only 40% of presumptive positive immunoassay compounds were confirmed by mass spectrometry, with immunoassays over detecting THC and under detecting cocaine exposure. After LC-MS/MS implementation, the nursery positivity rate decreased from 37% presumptive positive by immunoassay to 18% positive by LC-MS/MS, supporting the value of definitive, lower-threshold, broader-spectrum testing when neonatal or pediatric toxicology results may influence clinical or social decisions.
Perinatal and neonatal toxicology testing is evolving as laboratories aim to improve sensitivity, specificity, and detection of emerging novel psychoactive substances (NPS). Compared with traditional Tier-I immunoassays, Tier-II LC-MS/MS can expand compound coverage and increase diagnostic confidence in selected scenarios. However, deploying rapid Tier-II mass spectrometry testing requires substantial infrastructure, including specialized instrumentation, trained staff, thorough assay validation, robust quality control, and ongoing maintenance.
Mass spectrometry–based testing has important limitations as well. Targeted methods only detect analytes included in the panel, and laboratories may differ in compound coverage and reporting cutoffs. Definitive turnaround time may also be extended when specimens are sent to reference laboratories.
Interpreting results in the context of medications
Neonatal toxicology interpretation should account for medications administered during labor, delivery, and newborn care. For example, fentanyl used for labor epidural analgesia can lead to positive maternal or neonatal toxicology findings.7 Likewise, drugs given directly to the newborn may later be detected in meconium or umbilical cord specimens. Accordingly, results should be reviewed alongside maternal medication history, delivery records, neonatal medication administration, and the clinical presentation.
Addressing standardization and equity in newborn drug testing
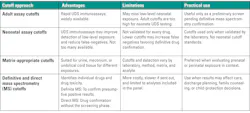
The literature also highlights the need for standardized protocols and attention to potential inequities in newborn drug testing. Racial and ethnic disparities have been reported in neonatal toxicology testing and subsequent involvement of child protective services.8 Laboratories and clinical teams should therefore ensure testing criteria are objective, standardized, and clinically justified. Cutoffs for presumptive positive/negative classification and for triggering confirmatory testing should be appropriate for both adult and neonatal populations (See Table 3). Future developments may include expanded high-resolution mass spectrometry, improved detection of NPS, and more portable analytical platforms. Nevertheless, Tier-I immunoassays will likely remain widely used for initial screening in many institutions because they are simpler to operate and offer rapid turnaround times.
Conclusion
In summary, Tier-I immunoassay based toxicology testing remains a useful screening approach in perinatal and neonatal care, but results are presumptive and subject to analytical limitations.1,3,5 Definitive Tier-II GC-MS and LC-MS/MS testing provides greater specificity and sensitivity and is particularly important when findings may affect patient management, neonatal evaluation, family counseling, or child-protection decisions.6 Method selection should reflect the clinical question, institutional resources, and an informed understanding of assay limitations and cutoff values used.
References
- McMillin GA, Morad AW, Boyd JM, et al. Biological testing and interpretation of laboratory results associated with detecting newborns with substance exposure. Clin Chem. 2024;70(7):934-947. doi:10.1093/clinchem/hvae018.
- Ryan EL. Interpreting toxicology results in perinatal and newborn specimens: Urine, meconium, and umbilical cord. Clin Lab Med. 2025;45(2):259-269. doi:10.1016/j.cll.2025.01.009.
- Saitman A, Fitzgerald RL, Lund K. Review: False positive urine drug screens. J Anal Toxicol. Published online 2026. doi:10.1093/jat/bkag007.
- Mullins GR, Reeves A, Yu M, Goldberger BA, Bazydlo LAL. Improved clinical sensitivity of a reflexive algorithm to minimize false-negative test results by a urine benzodiazepine immunoassay screen. J Appl Lab Med. 2018;2(4):555-563. doi:10.1373/jalm.2017.024539.
- Snozek CLH, Krasowski MD, Colby JM, et al. ADLM guidance document on laboratory testing for drugs of misuse to support the emergency department. J Appl Lab Med. 2026;11(1):155-180. doi:10.1093/jalm/jfaf172.
- Tesfazghi MT, Bardelmeier R, Saunders AN, et al. Development and implementation of one-step, broad-spectrum, high-sensitivity drug screening by tandem mass spectrometry in a pediatric population. J Appl Lab Med. 2022;7(2):409-420. doi:10.1093/jalm/jfab157.
- Siegel MR, Mahowald GK, Uljon SN, et al. Fentanyl in the labor epidural impacts the results of intrapartum and postpartum maternal and neonatal toxicology tests. Am J Obstet Gynecol. 2023;228(6):741.e1-741.e7. doi:10.1016/j.ajog.2022.11.1293.
- Schoneich S, Plegue M, Waidley V, et al. Incidence of newborn drug testing and variations by birthing parent race and ethnicity before and after recreational cannabis legalization. JAMA Netw Open. 2023;6(3):e232058. doi:10.1001/jamanetworkopen.2023.2058.
About the Author

Faon Rodriguez, MS
has over four decades of experience in clinical chemistry and research. A former supervisor for AdventHealth Laboratories, he is enjoying retirement and per diem collaboration with chemistry instrumental validations at AdventHealth.

Dexter Charles Mangio, BSMT, MT(AMT), MLS(FL DOH)
is a dedicated laboratory supervisor with over 20 years of professional experience in his field. A resident of Central Florida, Dexter enjoys spending his time outside of work with his family.