Molecular diagnostics for sensitive detection of dermatomycosis species

Dermatomycosis of the hair, skin, or nails is one of the most prevalent fungal infections worldwide, affecting 20–25% of the global population.1 The condition is caused by keratinolytic fungi called dermatophytes, in addition to molds and yeasts.2 Dermatophytes are classified into six pathogenic genera: Microsporum, Trichophyton, Epidermophyton, Nannizzia, Lophophyton, and Arthroderma. Additionally, dermatophytes are categorized as anthropophilic, zoophilic, or geophilic according to their natural habitat.3
Clinical presentation varies depending on the site of infection, type of fungus, and immune response of a patient but frequently include rash, itchy skin, hair loss, or thickened nails.3 Although antifungal medications are effective, dermatomycosis remains undertreated.4 In addition to causing permanent damage to the affected area, dermatomycosis can progress to severe disease in elderly and immunocompromised patients if left untreated.5-7 Furthermore, improper treatment will not only fail to clear the infection and prevent further spread but may also contribute to the development of antifungal resistance.5 Importantly, healthcare providers must first identify the fungal species causing infection to prescribe the most effective treatment.
Dermatomycosis can be difficult to diagnose clinically, as symptoms may resemble other skin disorders.8 Therefore, laboratory diagnostics are required for a definitive diagnosis. While traditional dermatomycosis diagnostics may take several weeks or are unable to identify dermatophyte species, molecular methods facilitate quick, species-specific determination.
Conventional diagnostics
Fungal Culture: Fungal culture using hair, skin, or nail specimens is a common method for detecting dermatomycosis and identifying fungal species.9 Culture involves plating and incubating the patient sample for 4–6 weeks in sample media. Fungal species can then be visually identified based on morphological characteristics such as colony size, pigmentation, shape, and type of growth.9 However, accurate species identification based on colony morphology requires well-trained mycology staff. While culture allows the identification of fungal species, the long incubation time delays species identification and subsequent treatment.
Additionally, fungal culture has limited sensitivity for detection of dermatomycosis. Some fungal species do not grow in culture, and recent systemic or topical use of antifungal treatments can prevent fungi from growing.2 In these cases, a sample is at risk of being incorrectly identified as negative. False negative results may also stem from improper specimen collection or insufficient sample material, whereas false positives may result from contamination.9
Microscopy: Direct microscopy of hair, skin, and nail specimens is commonly performed to assess the presence or absence of pathogenic fungi. As with culture, technical expertise is required to differentiate between dermatophytes, molds, and yeasts.9 While microscopy is less time-intensive than fungal culture, microscopy cannot be used to identify fungal species or indicate viability of the pathogen. Furthermore, microscopy has a high false negative rate of 35% for the diagnosis of dermatomycosis.10
Prior to microscopic evaluation, specimens are often digested in 10–20% potassium hydroxide (KOH), used as a clearing agent.11 This technique facilitates the visualization of hyphae and spores by digesting the keratin surrounding the fungi. However, usage of KOH preparation may lead to false negative results in 5–15% of cases.3 Additional stains, such as Calcofluor White (CW), can be used to improve sensitivity.12 Periodic acid-Schiff (PAS) staining is another common method for detection of fungal pathogens. PAS staining reacts with aldehyde groups in fungal cell wells, allowing visualization of hyphae and yeast-forms of fungi. Previous work has shown that for diagnosis of onychomycosis (OM), nail plate biopsy with PAS stain is more sensitive than culture, KOH preparation, and CW stain.13
Molecular diagnostics
Molecular methods for dermatomycosis diagnosis include polymerase chain reaction (PCR), real-time PCR, DNA microarray, and next-generation sequencing (NGS). These techniques involve direct detection of genetic material and provide a faster, more accurate alternative to conventional diagnostics. Importantly, molecular methods enable rapid identification of fungal species, which allows patients to receive more expedient and appropriate treatments.
PCR: Polymerase chain reaction (PCR)-based assays use primers to amplify fungi-specific DNA sequences in a sample.14,15 Primers target components of a fungi’s genome, including the nontranscribed spacer (NTS) regions, metalloprotease gene, chitin synthase (CHS) gene, tubulin gene, promoter region within ribosomal intergenic spacer, transcription elongation factor 1, actin gene, and calmodulin gene.9 Notably, PCR is 20–30% more specific than culture and is capable of detecting dermatophytes that are difficult to grow in culture.11
Nested PCR aims to increase sensitivity or specificity by using two sets of primers in two sequential amplification reactions; the product from the first reaction serves as the template for the second run.16 Prior work has found improved sensitivity for dermatophyte detection with nested PCR using CHS primers compared to conventional PCR.17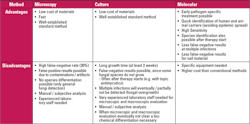
Real-time PCR: Real-time PCR provides rapid quantitative results for the identification of DNA or RNA, allowing estimation of a sample’s fungal load.18 Previous work has found that real-time PCR using a pan-dermatophyte primer targeting CHS is more sensitive (93%) than nested PCR (73.3%) targeting the same gene.19 Additionally, real-time PCR demonstrated higher sensitivity and specificity compared to microscopy with KOH. Real-time PCR showed a sensitivity of 93.3% and specificity of 40%, whereas KOH microscopy had a sensitivity of 80% and specificity of 16%.19
DNA microarray direct detection: PCR-based detection by DNA microarray enables direct, species-specific detection of fungal pathogens. DNA microarray methodology allows for multiplexing, enabling simultaneous detection of different species. While traditional PCR usually identifies 1 to 6 fungal species at a time,20 one commercially available PCR-based DNA microarray kit provides direct detection of 50 dermatophytes, with 23 species-specific dermatophytes in addition to six yeasts and molds within approximately three hours.21
Previous work comparing detection methods for OM and tinea pedis (TP) fungal infections found that the highest sensitivity among methodologies was PCR-based DNA microarray technology, with a sensitivity of 79% for OM and 91% for TP.22 In contrast, direct microscopy showed sensitivities of 68% for OM and 37% for TP. Fungal culture had the lowest sensitivities, 29% for OM and 44% for TP.22
The same study found that combining conventional diagnostic methods with PCR-based DNA microarray yielded the higher sensitivities. While combination of culture and direct microscopy resulted in fairly low sensitivities of 79% and 59% for OM and TP respectively, the combination of culture and DNA microarray increased sensitivity to 87% for OM and 94% for TP. Additionally, combining direct microscopy and DNA microarray achieved sensitivity of 92% for OM and 96% for TP.22 Overall, the combination of PCR-based DNA microarray methodology with direct microscopy yields sensitivity nearing 100% with the added benefits of species identification and a short turnaround time for results.
Next-generation sequencing: Next-generation sequencing (NGS) compares nucleotides in a sample against a catalogue library. NGS allows high throughput, rapid turnaround time, and accurate detection. Additionally, previous work has found that NGS is significantly more sensitive than culture for the detection of bacterial and fungal infections (95% versus 60%).23 The genome sequences of several species are available, including T. rubrum, Arthroderma vanbreuseghemii, A. benhamiae, and T. verrucosum.24,25 However, because NGS requires a genomic library, false negative results can occur if the library does not include the causative pathogen.
Advantages of molecular versus conventional methods
Species identification is crucial to appropriately treat patients with dermatomycosis. Differential diagnosis from noninfectious disorders is critical because they require different treatments.26 Additionally, dermatophyte or non-dermatophyte species identification is also essential for determining the optimal treatment and its duration.27,28 Providing an inappropriate treatment can lead to longer treatments with potential side effects. Furthermore, identification of the fungal species and antifungal susceptibility testing lowers the chance of resistance development.27,29,30
Direct detection with molecular methods enables rapid identification of fungal species, including those that are difficult to grow in culture. Molecular testing offers a faster turnaround time from collection to results, allowing for more expedient initiation of treatment.
Molecular methods also have the advantage of improved sensitivity compared to conventional diagnostics. A recent study by Pospischil, et al. 202226 examined specimens with a positive result by direct microscopy but a negative or contaminated culture. They showed that molecular methods were able to identify a fungal pathogen in 65% of these samples, emphasizing the importance of molecular testing for the diagnosis of dermatophyte and non-dermatophyte dermatomycosis when a culture yields a negative or contaminated result.26
Conclusion
Although dermatomycosis is the most prevalent fungal infection worldwide,1 it remains undertreated.4 While dermatomycosis generally has a low mortality rate and mild severity in healthy individuals, invasive dermatomycosis can cause severe disease in elderly and immunocompromised patients.5-7 Fungal culture and microscopy are commonly used to diagnose dermatomycosis, but methodological limitations such as long incubation time, limited sensitivity, and inability to identify fungal species can prevent patients from receiving timely and accurate diagnoses and treatments. However, the use of molecular methods facilitates rapid, species-specific determination of causative pathogens. In addition, the combination of molecular methods and conventional diagnostics leads to improved sensitivity for detection of dermatomycosis. Notably, the use of PCR-based DNA microarray methodology combined with direct microscopy results in 100% sensitivity and rapid species identification, thereby enabling patients to receive prompt and accurate treatment.
REFERENCES
1. Havlickova B, Czaika VA, Friedrich M. Epidemiological trends in skin mycoses worldwide. Mycoses. 2008;51 Suppl 4:2-15. doi:10.1111/j.1439-0507.2008.01606.x.
2. Nenoff P, Kruger C, Schaller J, Ginter-Hanselmayer G, Schulte-Beerbuhl R, Tietz HJ. Mycology - an update part 2: dermatomycoses: clinical picture and diagnostics. J Dtsch Dermatol Ges. 2014;12(9):749-777. doi:10.1111/ddg.12420.
3. Weitzman I, Summerbell RC. The dermatophytes. Clin Microbiol Rev. 1995;8(2):240-259. doi:10.1128/CMR.8.2.240.
4. Lipner SR, Joseph WS, Vlahovic TC, et al. Therapeutic Recommendations for the Treatment of Toenail Onychomycosis in the US. J Drugs Dermatol. 2021;20(10):1076-1084. doi:10.36849/JDD.6291.
5. Achterman RR, White TC. A foot in the door for dermatophyte research. PLoS Pathog. 2012;8(3):e1002564. doi:10.1371/journal.ppat.1002564.
6. Wang R, Huang C, Zhang Y, Li R. Invasive dermatophyte infection: A systematic review. Mycoses. 2021;64(4):340-348. doi:10.1111/myc.13212.
7. Zhu A, Zembower T, Qi C. Molecular detection, not extended culture incubation, contributes to diagnosis of fungal infection. BMC Infect Dis. 2021;21(1):1159. doi:10.1186/s12879-021-06838-6.
8. Yadgar RJ, Bhatia N, Friedman A. Cutaneous fungal infections are commonly misdiagnosed: A survey-based study. J Am Acad Dermatol. 2017;76(3):562-563. doi:10.1016/j.jaad.2016.09.041.
9. Heckler I, Sabalza M, Bojmehrani A, Venkataraman I, Thompson C. The need for fast and accurate detection of dermatomycosis. Med Mycol. 2023;61(5). doi:10.1093/mmy/myad037.
10. Petrucelli MF, Abreu MH, Cantelli BAM, et al. Epidemiology and Diagnostic Perspectives of Dermatophytoses. J Fungi (Basel). 2020;6(4). doi:10.3390/jof6040310.
11. Kidd SE, Weldhagen G. Diagnosis of dermatophytes: from microscopy to direct PCR. Microbiol Aust. 2022;43(1):9-13. doi:10.1071/ma22005.
12. Abdelrahman T LBV, Waller J, Noacco G, Candolfi E. Dermatomycosis: comparison of the performance of calcofluor and potassium hydroxide 30% for the direct examination of skin scrapings and nails. J Mycol Med. 2006;16(2):87-91. doi:10.1016/j.mycmed.2006.03.003.
13. Weinberg JM, Koestenblatt EK, Tutrone WD, Tishler HR, Najarian L. Comparison of diagnostic methods in the evaluation of onychomycosis. J Am Acad Dermatol. 2003;49(2):193-197. doi:10.1067/s0190-9622(03)01480-4.
14. Liu D, Coloe S, Baird R, Pedersen J. Application of PCR to the identification of dermatophyte fungi. J Med Microbiol. 2000;49(6):493-497. doi:10.1099/0022-1317-49-6-493.
15. Brillowska-Dabrowska A, Saunte DM, Arendrup MC. Five-hour diagnosis of dermatophyte nail infections with specific detection of Trichophyton rubrum. J Clin Microbiol. 2007;45(4):1200-1204. doi:10.1128/JCM.02072-06.
16. Green MR, Sambrook J. Nested Polymerase Chain Reaction (PCR). Cold Spring Harb Protoc. 2019;2019(2). doi:10.1101/pdb.prot095182.
17. Garg J, Tilak R, Singh S, et al. Evaluation of pan-dermatophyte nested PCR in diagnosis of onychomycosis. J Clin Microbiol. 2007;45(10):3443-3445. doi:10.1128/JCM.02367-06.
18. Ohst T, Kupsch C, Graser Y. Detection of common dermatophytes in clinical specimens using a simple quantitative real-time TaqMan polymerase chain reaction assay. Br J Dermatol. 2016;174(3):602-609. doi:10.1111/bjd.14198.
19. Emam SM, Abd El-salam OH. Real-time PCR: A rapid and sensitive method for diagnosis of dermatophyte induced onychomycosis, a comparative study. Alex J Med. 2016;52(1):83-90. doi:10.1016/j.ajme.2015.05.001
20. Verrier J, Monod M. Diagnosis of Dermatophytosis Using Molecular Biology. Mycopathologia. 2017;182(1-2):193-202. doi:10.1007/s11046-016-0038-z.
21. Gosink J. Dermatomycosis diagnostics by DNA MICROARRAY. 2022.
22. Bieber K, Harder M, Stander S, et al. DNA chip-based diagnosis of onychomycosis and tinea pedis. J Dtsch Dermatol Ges. 2022;20(8):1112-1121. doi:10.1111/ddg.14819.
23. Chen P, Sun W, He Y. Comparison of the next-generation sequencing (NGS) technology with culture methods in the diagnosis of bacterial and fungal infections. J Thorac Dis. 2020;12(9):4924-4929. doi:10.21037/jtd-20-930.
24. Alshahni MM, Yamada T, Yo A, et al. Insight into the draft whole-genome sequence of the dermatophyte Arthroderma vanbreuseghemii. Sci Rep. 2018;8(1):15127. doi:10.1038/s41598-018-33505-9.
25. Martinez DA, Oliver BG, Graser Y, et al. Comparative genome analysis of Trichophyton rubrum and related dermatophytes reveals candidate genes involved in infection. mBio. 2012;3(5):e00259-00212. doi:10.1128/mBio.00259-12.
26. Pospischil I, Reinhardt C, Bontems O, et al. Identification of Dermatophyte and Non-Dermatophyte Agents in Onychomycosis by PCR and DNA Sequencing-A Retrospective Comparison of Diagnostic Tools. J Fungi (Basel). 2022;27;8(10):1019. doi:10.3390/jof8101019.
27. Silva LB, de Oliveira DB, da Silva BV, et al. Identification and antifungal susceptibility of fungi isolated from dermatomycoses. J Eur Acad Dermatol Venereol. 2014;28(5):633-640. doi:10.1111/jdv.12151.
28. Ely JW, Rosenfeld S, Seabury Stone M. Diagnosis and management of tinea infections. Am Fam Physician. 2014;90(10):702-710.
29. Berkow EL, Lockhart SR, Ostrosky-Zeichner L. Antifungal Susceptibility Testing: Current Approaches. Clin Microbiol Rev. 2020;29;33(3):e00069-19. doi:10.1128/CMR.00069-19.
30. Martinez-Rossi NM, Bitencourt TA, Peres NTA, et al. Dermatophyte Resistance to Antifungal Drugs: Mechanisms and Prospectus. Front Microbiol. 2018;9:1108. doi:10.3389/fmicb.2018.01108.
About the Author

Jackie Weiss, PhD
is the Scientific Affairs Liaison at EUROIMMUN US (part of Revvity). Her role includes working with key opinion leaders on scientific collaborations, scientific writing, and supporting the team with commercial activities.