Diagnostic stewardship and molecular assays: A laboratorian’s primer

Over the last few decades, the healthcare system in the United States has gradually transitioned from a fee-for-service to a value-based payment model.1 This has led healthcare organizations to look for ways to optimize medical services they offer in order to deliver improved patient outcomes more cost effectively. Diagnostic stewardship (DxS) is a useful tool to accomplish this task. DxS is the development and application of processes that optimize the use of clinical laboratory testing to improve the diagnosis and subsequent treatment decisions in medical practice.2-4 Simply: Use the right test for the right patient prompting the right action at the right time.5,6 Although DxS can occur in all stages of testing, the bulk of successful interventions occurs in the preanalytical phase with limited opportunities in the analytical/postanalytical phases of testing.2-4 This can make implementation challenging as the bulk of preanalytical processes (e.g., test decision-making/ordering and specimen collection/transport) occur outside of the laboratory.4 Close collaboration with non-laboratorian clinical stakeholders is necessary to make substantial changes to institutional practices that impact test selection, ordering, and specimen collection/transportation.3
Molecular assays are likely to deliver the most return on DxS. Molecular testing utilizes genetic information to diagnose disease etiologies, most notably in infectious diseases and oncology. Although molecular testing often has advantages over comparator methods, there are limitations that are underrecognized, leading to negative patient outcomes and significant laboratory costs. Given this, they are excellent candidates for DxS. The purpose of this article is to deliver a practical overview and a pragmatic approach for the development of molecular DxS interventions at the highest yield stage of testing, the preanalytical stage.
Diagnostic stewardship principles
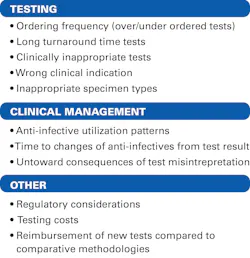
One of the most important, yet challenging, steps when implementing DxS interventions is test assessment.3 It is important to select tests that will yield the highest benefit. The initial step in assessment should be the identification of several candidate tests followed by a rigorous review of institutional data. Potential key areas for data collection to guide which tests to evaluate require close scrutiny (Figure 1).3 High-level discussion with key clinical stakeholders is instrumental to successful identification of high-priority tests following data acquisition.3 Review of this data with key stakeholders is important to ensure the input of the end users is considered prior to implementation of DxS interventions.2-4 Ideally, the composition of stakeholders should include laboratory administration, common clinical users of the testing (both generalists and specialists), healthcare units dependent on the testing results (e.g., antimicrobial stewardship, infection control, information technology, and executive hospital leadership).2-4,7 Further discussions and collaborations with these same stakeholders are key following test selection to ensure successful implementation and monitoring of DxS interventions.3
Pre-analytical interventions lead to downstream success
Following test selection, determining which DxS activity should be implemented is the next challenge. For preanalytical interventions, the most effective measures are focused on optimizing testing decision-making processes.8 Clinician education should be emphasized.2,3 Digitally enabled clinical decision support tools can be effective in guiding appropriate test ordering.9,10 Careful selection of diagnostic tests for use in institutional order sets, and use of best practice alerts during order entry can limit non-indicated testing.6 The use of nudges (educational pop-ups) and framing comments (comments highlighting the positive/negative impact of the test) can be highly effective as well.4,6 In some situations, testing restrictions through cascading (stepwise testing) or conditional (strict testing requirements) can be used to reduce non-indicated testing; however, this could lead to unintended restrictions on indicated orders.4,6 When deploying testing restrictions using these methods, it is important to have the ability to offer streamlined pathologist consultation.2,3,6 For testing that can be challenging to interpret and may result in adverse treatment decisions, strict restrictions can be implemented where orders can only be placed and/or need approval from experts with the knowledge of the testing limitations and with the ability to interpret the results.3,11 This can be accomplished by restricting tests to certain specialties or developing a multi-specialty DxS committee.3,11 Restrictive methods are increasingly employed in molecular testing due to the challenges in interpreting results and increased costs associated with them (e.g., direct test costs, lack of payor reimbursement, unnecessary healthcare resources due to improper interpretation).3,11 DxS interventions for analytic stages of testing are generally centered around ensuring the testing methodology used is the best for the patient population served and clinical performance by the laboratory meets regulatory standards.2-4 Postanalytical stewardship interventions should ensure proper interpretation of results by clinicians and appropriate follow-up testing is performed.2-4
Ongoing feedback with non-laboratorians is key
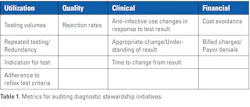
DxS programs are not only most successful when there is multidisciplinary collaboration, but also excel when ongoing clinician education and continuous monitoring with feedback are incorporated.4 Three domains should be considered when deciding which metrics to measure and report to key stakeholders: utilization, diagnostic performance, and clinical impact. These metrics serve as benchmarks informing the success of the intervention. Data collection is about quality, not quantity. The right data should reflect clinical decision-making quality, appropriate test utilization, and downstream clinical impact. These metrics may be the same or similar to those collected when determining which candidate tests would be the focus of DxS action (Table 1).
The post go-live phase is where many programs can quietly fail because they stop measuring the right things. A DxS program is ultimately considered successful when it reduces inappropriate testing, improves diagnostic yield, and positively impacts clinical management without missing disease. This requires continuous monitoring of utilization, yield, appropriateness, and clinical outcomes using structured LIS/EHR data and targeted chart review. If testing volumes do not change, it may mean the intervention is being bypassed. Conversely, if the intervention is working as intended, it is important to ensure that stable or rising testing volumes are driven by appropriate clinical use, such as shifts in local epidemiology.
DxS in practice: Multiplex PCR for gastroenteritis
The rapid adoption and proliferation of multiplex PCR (mPCR) syndromic panels are a great example of how DxS can improve clinical practice. mPCR gastrointestinal (GI) panels are high-performing tools, but without stewardship, they may lead to clinical confusion and excessive laboratory costs. The panels have broad detection of microorganisms, and there is data which supports that these assays have enhanced diagnostic yield and return results more quickly than conventional tests.12-17 These assays have shifted the bottleneck from detection to interpretation and appropriate utilization. Limitations of these assays include the inability to differentiate between active infection, asymptomatic colonization, and prolonged shedding of nucleic acid. Some laboratories have developed guidelines to aid clinicians in proper test utilization. These laboratories may utilize duration of illness or other clinical features (e.g., bloody diarrhea, fever, or prolonged duration) to guide clinicians towards testing.18 For patients with hospital-onset diarrhea who have been hospitalized for more than three days, testing by mPCR is generally restricted given the low likelihood of pathogen identification and the risk for Clostridioides difficile detection indicating colonization instead of active infection.19,20 Ultimately, optimizing GI testing requires DxS that aligns test utilization with clinical presentation, patient risk factors, and the likelihood of actionable results; maximizing clinical impact while minimizing unnecessary costs, inappropriate treatment, and diagnostic uncertainty.
DxS in practice: Multiplex PCR for central nervous system infections
When testing cerebrospinal fluid (CSF) specimens utilizing mPCR panels, it is important to note that this is purely adjunctive. Molecular testing is not intended to replace conventional culture and targeted assays for pathogens with high pre-test probability. The strongest pre-analytic measure to screen specimens is requiring objective evidence that demonstrates central nervous system inflammation. Several studies have shown that restricting testing to CSF with demonstrable pleocytosis results in decreased utilization of these assays while showing an increase in test positivity, especially for bacterial pathogens.21-24 Notably, some viral infections may occur without CSF pleocytosis in specific patient populations (e.g., immunocompromised with neutropenia) and stewardship strategies should combine CSF parameters with clinical context rather than rely on white blood count thresholds alone.
Evolving molecular tests may require evolving DxS strategies
As molecular technology continues to evolve, clinical laboratorians should not only employ these same prudent DxS strategies, but may need to adapt to unique practices as they develop. Next-generation sequencing (NGS) methods are appealing diagnostic solutions due to the exponential increase in the number of pathogens detected compared to fixed mPCR panels and traditional culture; however, few laboratories have the capability to complete NGS testing in-house.25 While formal utilization guidance is currently unavailable, best practice strategies are emerging. As noted above, clinical microbiologists, infectious disease physicians, and pathologists should build a framework in the pre-analytical phases for developing guidance to identify clinical scenarios, patient populations, sample types, and tiered diagnostic testing to guide optimal NGS testing.3,25-27 Naureckas-Li recently described a collaborative process to determine institutional consensus of NGS using a modified Delphi approach that can be instructional for centers incorporating NGS testing.27 Additional considerations include clinician awareness of organisms on targeted NGS menus, optimal collection timing, detection of nonpathogenic organisms increasing diagnostic uncertainty, delayed turnaround time, and testing reimbursement.25,26
Conclusion
DxS is essential for clinical laboratories navigating the myriad of clinical advantages alongside the increasing complexities and costs of molecular diagnostics. By leading stewardship efforts with clinicians and health system leadership in the pre-analytical phases of testing, clinical laboratorians are uniquely positioned to influence diagnostic accuracy, patient management, and healthcare value. As molecular technologies expand, laboratorians must continue to embrace DxS ensuring that the right innovative tools are used thoughtfully and equitably at the right time for the right patient prompting the right action.
References
- Rooke-Ley H, Song Z, Zhu JM. Value-based payment and vanishing small independent practices. JAMA. 2024;332(11):871-872. doi:10.1001/jama.2024.12900.
- Dumm RE, Marlowe EM, Patterson L, et al. The foundation for the microbiology laboratory's essential role in diagnostic stewardship: An ASM Laboratory Practices Subcommittee report. J Clin Microbiol. 2024;62(10):e0096024. doi: 10.1128/jcm.00960-24.
- Valencia-Shelton F, Anderson N, Palavecino EL, et al. Approaches to developing and implementing a molecular diagnostics stewardship program for infectious diseases: An ASM Laboratory Practices Subcommittee report. J Clin Microbiol. 2024;62(11):e0094124. doi:10.1128/jcm.00941-24.
- Fabre V, Davis A, Diekema DJ, et al. Principles of diagnostic stewardship: A practical guide from the Society for Healthcare Epidemiology of America Diagnostic Stewardship Task Force. Infect Control Hosp Epidemiol. 2023;44(2):178-185. doi:10.1017/ice.2023.5.
- Siragusa LM, Gamba M, Wertli MM, Hug B. Exploring the role of diagnostic stewardship concepts outside of antimicrobial stewardship: protocol for a scoping review. BMJ Open. 2026;16(3):e110621. doi:10.1136/bmjopen-2025-110621.
- Coffey KC, Claeys K, Morgan DJ. Diagnostic stewardship for urine cultures. Infect Dis Clin North Am. 2024;38(2):255-266. doi:10.1016/j.idc.2024.03.004.
- Claeys KC, Coffey KC, Morgan DJ. What is diagnostic stewardship? J Appl Lab Med. 2025;10(1):130-139. doi:10.1093/jalm/jfae130.
- Hitchcock MM, Gomez CA, Pozdol J, Banaei N. Effective approaches to diagnostic stewardship of syndromic molecular panels. J Appl Lab Med. 2024;9(1):104-115. doi:10.1093/jalm/jfad063.
- Georgiou A, Li J, Hardie RA, et al. Diagnostic informatics-The role of digital health in diagnostic stewardship and the achievement of excellence, safety, and value. Front Digit Health. 2021;3:659652. doi:10.3389/fdgth.2021.659652.
- Li J, Thomas J, Baysari M, Georgiou A, Prgomet M. Diagnostic stewardship mechanisms in electronic test results management - A scoping review. Int J Med Inform. 2026;207:106178. doi:10.1016/j.ijmedinf.2025.106178.
- Baghdadi JD, O'Hara LM, Johnson JK, et al. Diagnostic stewardship to support optimal use of multiplex molecular respiratory panels: A survey from the Society for Healthcare Epidemiology of America Research Network. Infect Control Hosp Epidemiol. 2023;44(11):1823-1828. doi:10.1017/ice.2023.72.
- Gu Z, Zhu H, Rodriguez A, et al. Comparative evaluation of broad-panel PCR assays for the detection of gastrointestinal pathogens in pediatric oncology patients. J Mol Diagn. 2015;17(6):715-21. doi:10.1016/j.jmoldx.2015.06.003.
- Buss SN, Leber A, Chapin K, et al. Multicenter evaluation of the BioFire FilmArray gastrointestinal panel for etiologic diagnosis of infectious gastroenteritis. J Clin Microbiol. 2015;53(3):915-25. doi:10.1128/JCM.02674-14.
- Szymczak WA, Engsbro AL, Lisby JG, et al. Multicenter evaluation of the QIAstat-Dx Gastrointestinal Panel 2, a multiplex PCR platform for the diagnosis of acute gastroenteritis. J Clin Microbiol. 2025;63(8):e0198324. doi:10.1128/jcm.01983-24.
- Ambrosius-Eichner J, Hogardt M, Berger A, et al. Comparative evaluation of the detection rate, workflow and associated costs of a multiplex PCR panel versus conventional methods in diagnosis of infectious gastroenteritis. J Med Microbiol. 2024;73(2)doi:10.1099/jmm.0.001795.
- Cybulski RJ, Jr., Bateman AC, Bourassa L, et al. Clinical impact of a multiplex gastrointestinal polymerase chain reaction panel in patients with acute gastroenteritis. Clin Infect Dis. 2018;67(11):1688-1696. doi:10.1093/cid/ciy357.
- Moon RC, Bleak TC, Rosenthal NA, et al. Relationship between diagnostic method and pathogen detection, healthcare resource use, and cost in U.S. adult outpatients treated for acute infectious gastroenteritis. J Clin Microbiol. 2023;61(2):e0162822. doi:10.1128/jcm.01628-22.
- Shane AL, Mody RK, Crump JA, et al. 2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea. Clin Infect Dis. 2017;65(12):1963-1973. doi:10.1093/cid/cix959.
- Miller JM, Binnicker MJ, Campbell S, et al. Guide to utilization of the microbiology laboratory for diagnosis of infectious diseases: 2024 update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). Clin Infect Dis. 2024:ciae104. doi:10.1093/cid/ciae104.
- Hitchcock MM, Gomez CA, Banaei N. Low yield of FilmArray GI Panel in hospitalized patients with diarrhea: An opportunity for diagnostic stewardship intervention. J Clin Microbiol. 2018;56(3):e01558-17. doi:10.1128/JCM.01558-17.
- Broadhurst MJ, Dujari S, Budvytiene I, et al. Utilization, yield, and accuracy of the FilmArray Meningitis/Encephalitis panel with diagnostic stewardship and testing algorithm. J Clin Microbiol. 2020;58(9):e00311-20. doi:10.1128/JCM.00311-20.
- Erba A, Franzeck FC, Hinic V, Egli A, Osthoff M. Utilization of a Meningitis/Encephalitis PCR panel at the University Hospital Basel - A retrospective study to develop a diagnostic decision rule. Front Med (Lausanne). 2024;11:1351903. doi:10.3389/fmed.2024.1351903.
- McCreery R, Nielsen L, Clarey D, Murphy C, Van Schooneveld TC. Evaluation of cerebrospinal fluid white blood cell count criteria for use of the BioFire(R) FilmArray(R) Meningitis/Encephalitis Panel in immunocompromised and nonimmunocompromised patients. Diagn Microbiol Infect Dis. 2022;102(3):115605. doi:10.1016/j.diagmicrobio.2021.115605.
- Ibrahim NH, Kinsella P, Chan E, Cronin K, Bond K. Efficient use of the BioFire(R) FilmArray(R) Meningitis/Encephalitis Panel: A diagnostic stewardship approach. Intern Med J. 2026;56(5):849-857. doi:10.1111/imj.70391.
- Gaston DC, Chiang AD, Dee K, et al. Diagnostic stewardship for next-generation sequencing assays in clinical microbiology: An appeal for thoughtful collaboration. Clin Lab Med. 2024;44(1):63-73. doi:10.1016/j.cll.2023.10.002.
- Filkins LM, Bryson AL, Miller SA, Mitchell SL. Navigating clinical utilization of direct-from-specimen metagenomic pathogen detection: Clinical applications, limitations, and testing recommendations. Clin Chem. 2020;66(11):1381-1395. doi:10.1093/clinchem/hvaa183.
- Naureckas Li C, Jhaveri R, Huston S. Results of a local modified Delphi consensus on use of plasma metagenomic next-generation sequencing. Infect Control Hosp Epidemiol. 2025;46(12):1275-1277. doi:10.1017/ice.2025.10334.
About the Author

John Emmanuel Markantonis, DO, D(ABMM), FASCP, FCAP
is a clinical pathologist at NYU Langone Health. He is passionate about improving patient care through diagnostic stewardship and responding to the emerging threat of antimicrobial resistance through antimicrobial stewardship.

Nicholas Moore, PhD, D(ABMM)
is the associate director of clinical microbiology and an associate professor at Rush University Medical Center in Chicago. His research interests are focused on antimicrobial resistance, diagnostic stewardship, and the implementation of innovative diagnostic technologies to improve patient care and laboratory practice.

Dusten T. Rose, PharmD, BCIDP, FIDSA
is a Medical Science Liaison in U.S. Medical Affairs at bioMérieux. He is a board-certified infectious diseases pharmacist with nearly 15 years of inpatient clinical experience. His interests include antimicrobial stewardship, clinical impact of emerging diagnostics, and antimicrobial resistance.