12 steps to CD4 testing Part II—HIV treatment

The 2016 and 2017 World Health Organization (WHO) guidelines provide guidance on the diagnosis of human immunodeficiency virus (HIV) infection, the care of people living with HIV, and the use of antiretroviral (ARV) drugs for treating and preventing HIV infection.
While these guidelines recommend lifelong antiretroviral therapy (ART) regardless of CD4 cell count (“treat all policy”) and analysis of viral load (VL) as the preferred monitoring approach, they also provide clear guidance on the indispensable role of CD4 in assessing baseline risk of disease progression—particularly for individuals presenting with advanced disease—decisions regarding starting and stopping prophylaxis for opportunistic infections (OIs), and prioritization decisions regarding ART initiation in settings where universal treatment is not possible. CD4 cell count measurement may also be important for people who are failing ART.
As a recap, the following copy is a continuation from last month’s “Part I: HIV Testing.”
3. PRIORITIZATION OF TREATMENT INITIATION
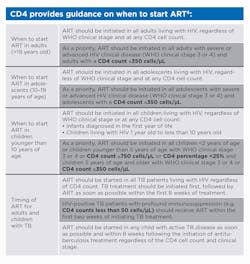
Prioritization of antiretroviral therapy (ART) initiation is outlined in the chart below entitled, “CD4 provides guidance on when to start ART.”6
4. RAPID INITIATION OF ART
Recommendation for rapid initiation of ART
People with no contraindication to rapid ART initiation should be fully informed of the benefits of ART and offered rapid ART initiation, including the option of same-day initiation.7
Rapid ART start is especially important for people with very low CD4 cell count, for whom the risk of death is high.7
Although no longer a requirement for ART initiation, baseline CD4 cell count testing should be performed to determine whether the patient has advanced HIV disease.7
5. DIAGNOSING TREATMENT FAILURE
Monitoring response to ART and diagnosing treatment failure in absence of viral load testing in individuals who are not stable on ART
Viral load is recommended as the preferred monitoring approach to diagnose and confirm treatment failure.8
If viral load testing is not routinely available, CD4 count and clinical monitoring should be used to diagnose treatment failure, with targeted viral load testing to confirm viral failure where possible.8
In settings where routine viral load monitoring is available, CD4 cell count monitoring can be stopped in individuals who are stable on ART and virally suppressed.8
A patient is considered stable on ART based on the following criteria:8 on ART for at least one year, no current illnesses, good understanding of lifelong adherence, and evidence of treatment success (two consecutive viral load measurements below 1,000 copies/ml).
6. IDENTIFYING IMMUNOLOGICAL FAILURE
The role of CD4 in identifying immunological failure
The 2016 WHO guidelines point out the role of CD4 in the identification of immunological failure for the decision to switch ART regimens:9
- Adults and adolescents: CD4 count at or below 250 cells/ul following clinical failure OR persistent CD4 levels below 100 cells µ/L
- Children younger than 5 years: Persistent CD4 levels below 200 cells µ/L
- Children older than 5 years: Persistent CD4 levels below 100 cells µ/L
10. TREATMENT ADHERENCE
Adherence support interventions
The 2016 WHO Guidelines strongly recommend to provide adherence support interventions to people on ART.16 The following interventions demonstrated benefit in improving adherence and viral suppression:16
- Peer counselors
- Mobile phone text messages
- Reminder devices
- Cognitive-behavioral skills training/medication adherence training
- Fixed-dose combinations and once-daily regime
Follow this space next month in MLO’s Special Feature for the final technical overview of Beckman Coulter Life Sciences’ “12 Steps to CD4 Testing.”
REFERENCES
6. World Health Organization (2016): Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection; recommendations for a public health approach – 2nd ed., page xxxi.
7. World Health Organization (2017): Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy, page 20.
8. World Health Organization (2016): Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection; recommendations for a public health approach – 2nd ed., page xxxiv.
9. World Health Organization (2016): Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection; recommendations for a public health approach – 2nd ed., page 131.1.
16. World Health Organization (2016): Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection; recommendations for a public health approach – 2nd ed., page xlii.
