From imaging to blood: Alzheimer’s diagnostics evolve
Alzheimer’s disease (AD) is the major cause of dementia worldwide that leads to morbidity, long‑term care utilization, and significant healthcare costs. At present, over 7 million Americans are living with AD which is projected to reach nearly 13 million by 2050.1 Health and long-term care costs for people living with dementia are projected to reach nearly $1 trillion in 2050.1
Dementia is caused due to damage or changes in the brain, dementia can also be caused due to other reasons including vascular dementia, Parkinson's disease, dementia with Lewy bodies, and frontotemporal dementia. Severe head injury and a few less common causes such as Huntington's disease, leukoencephalopathies, Creutzfeldt-Jakob disease, some cases of multiple sclerosis (MS) or amyotrophic lateral sclerosis (ALS), and multiple-system atrophy.2 With the emergence of newer therapies, accurate and earlier diagnosis has become increasingly important. Hence, laboratory testing, along with clinical evaluation, plays a very crucial role in confirming Alzheimer’s disease.
Evolution in AD diagnosis
The diagnosis of Alzheimer's disease has evolved from subjective, post-mortem autopsy examinations in the early 20th century to objective, biomarker-driven, and imaging-based techniques (amyloid PET, cerebrospinal fluid) that detect the disease in living patients decades before symptoms appear. This shift has enabled diagnosis in the preclinical stage rather than only at advanced dementia stages.
In November 1906, Dr. Alois Alzheimer, a clinical psychiatrist and neuroanatomist first reported this disease as “a peculiar severe disease process of the cerebral cortex” by identifying amyloid plaques and neurofibrillary tangles (NFTs) in brain tissue postmortem. His colleague and mentor, Emil Kraepelin subsequently named this disease as Alzheimer’s disease in 1910.3
In 1984, the National Institute of Neurological and Communicative Disorders and Stroke (NINCDS) and the Alzheimer’s Disease and Related Disorders Association (ADRDA) first standardized a diagnostic framework based on clinical, cognitive, and behavioral symptoms as: “Probable,” “Possible,” and “Definite.”4,5
In 2011, the National Institute on Aging (NIA) and the Alzheimer's Association (AA) convened three workgroups that published separate recommendations for the diagnosis and evaluation of Alzheimer's disease in its preclinical, mild cognitive impairment (MCI), and dementia phases.6-9 Biomarkers were incorporated into the diagnostic algorithm to facilitate early and more accurate detection. These biomarkers included amyloid (positron emission tomography) PET imaging, CSF Aβ42, CSF t-tau and p-tau, glucose metabolism on fluorodeoxyglucose PET, and characteristic patterns of cortical atrophy on structural MRI.6,8 Nevertheless, significant barriers to the use of biomarkers in clinical settings due to lack of standardization, variability in interpretation, and limited availability, led the NIA-AA criteria to not recommend biomarkers for routine diagnostic purposes.
Subsequently the Alzheimer's Association had a series of recommendations for AD diagnosis. In 2012, an NIA-AA workgroup published a consensus document on the neuropathologic diagnosis of AD;10,11 in 2018, they published a research framework; and in 2024, a revised criteria for diagnosis and staging of Alzheimer's disease were published.12,13 The 2018 research framework emphasized that it was intended solely for research purposes and not designed for clinical use.12 However, the 2024 diagnostic criteria are intended for use in actual clinical practice.13
Tests for diagnosing AD
Physicians use several diagnostic tools, medical history and other information, including neurological exams, cognitive and functional assessments, brain imaging (MRI, CT, PET) and cerebrospinal fluid or blood tests to make an accurate diagnosis for Alzheimer’s disease.14
Biomarkers for AD
Biomarkers can indicate early signs of AD and enable early intervention in the disease process. Biomarkers like amyloid PET imaging, CSF Aβ42, CSF t-tau and p-tau, glucose metabolism on fluorodeoxyglucose PET, and characteristic patterns of cortical atrophy on structural MRI were incorporated into the diagnostic algorithm in the NIA-AA 2011 recommendation. However, due to the lack of standardization, they were not recommended for routine diagnosis.6,8
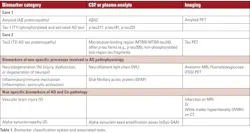
In the revised criteria for diagnosis and staging of AD published in 2024 by the Alzheimer’s Association, biomarkers were broadly classified as follows:15
(1) Core biomarkers of Alzheimer’s disease neuropathologic change (ADNPC)
(2) Non-specific biomarkers that are important in Alzheimer’s but are also involved in other brain diseases
(3) Biomarkers of diseases/conditions that commonly co-exist with Alzheimer’s/co-pathology
Table 1 lists the three classes of biomarkers and their associated tests.5 These tests have high accuracy in diagnosing the etiology of cognitive impairment, informing appropriate treatment and care planning, offering prognostic insights,16,17 and identifying eligibility for emerging amyloid-targeting therapies.18,19
Emergence of blood‑based biomarkers (BBMs)
Alzheimer's disease (AD) diagnosis traditionally relied on positron emission tomography (PET) with radiotracers that bind to amyloid plaques or insoluble tau aggregates, or on cerebrospinal fluid (CSF) assays that measure biomarkers like amyloid beta (Aβ)42, Aβ40, total tau (t-tau), and phosphorylated tau (p-tau).20 Despite the high diagnostic accuracy of these methods, PET scan is expensive and not widely available and the CSF test is both invasive and impractical for widespread use in clinical practice.21,22
Blood-based biomarkers (BBMs) have now emerged that are less expensive and more accessible and acceptable for patients compared to PET and CSF tests. Multiple BBMs—such as Aβ42/Aβ40 and tau phosphorylated at different sites (p-tau181, p-tau217, and p-tau231)—have been shown to strongly correlate with AD pathology.23 Additionally, BBMs are uniquely positioned to address the growing diagnostic demands driven by the introduction of amyloid-targeting therapies.24
Several BBM tests are now commercially available, however their diagnostic performance differs across assays,25,26 and their use in clinical settings remains unstandardized. Currently two FDA-cleared BBM tests are available for AD:
- Fujirebio’s Lumipulse G pTau217/β-Amyloid 1-42 plasma ratio test, which measures the ratio of specific tau (pTau217) and amyloid-beta (β-Amyloid 1-42) proteins in the plasma and is indicated for the early detection of amyloid plaques associated with Alzheimer’s disease in adult patients, aged 55 years and older, exhibiting signs and symptoms of the disease.27
- Elecsys pTau181 plasma test, developed by Roche, is intended for use in adult patients, aged 55 years and older, presenting with signs or symptoms of cognitive impairment. This tests assesses the likelihood of amyloid plaques to help primary care physicians determine which patients do not require Alzheimer’s-related follow-up tests, such as PET scans or cerebrospinal fluid analysis.28
Even though blood-based biomarkers are rapidly advancing, they are still not used as a standalone confirmatory test for AD diagnosis due to issues with low accuracy in diverse populations, lack of standardization, and high rates of false positives compared to gold-standard methods. That said, they are highly promising for screening or triaging and confirming Alzheimer’s diagnosis with robust methods like cerebrospinal fluid (CSF) analysis or PET scans.29, 30.
Dr. Yonghong Li and his colleagues at Quest Diagnostics performed a study to determine the efficacy and cost-effectiveness of using blood-based biomarker as a triage in Alzheimer’s disease testing. Dr. Michael K. Racke, Medical Director of Neurology at Quest Diagnostics and a co-investigator of this study summarized their findings as below:
“This research demonstrates the efficacy and cost-effectiveness of blood-based biomarker testing in assessing Alzheimer’s disease pathology. PET scans, which are often less accessible for many, are more expensive and invasive. In this study, we examined two methods of diagnosing patients with cognitive decline: performing blood testing before confirming diagnosis with a PET scan and proceeding straight to a PET scan without blood testing first. Results showed that, whether PET scans are limited or readily available, blood testing is still less expensive. This is why we believe the future of assessing risk or diagnosing AD will likely include a variety of testing modalities and biomarkers, including blood, to help clinicians identify patients in the early stages of disease progression.”
Conclusion
It can be expected that continued refinement and standardization of plasma assays with robust validation in diverse population powered by artificial intelligence (AI) to enable wider use of blood‑based biomarkers in primary care and community settings in the very near future. Moreover, with the rapid advancements in imaging technology coupled with AI, we can expect to see less expensive, portable imaging systems at the point-of-care to enable rapid and early diagnosis of Alzheimer’s disease.
References
- Alzheimer’s Association 2025 Alzheimer’s Disease Facts and Figures. Alzheimers Dement. 2025;21(5).
- Dementia Causes. Stanford Medicine Health Care. Accessed April 7, 2026. https://stanfordhealthcare.org/medical-conditions/brain-and-nerves/dementia/causes.html.
- Hippius H, Neundörfer G. The discovery of Alzheimer's disease. Dialogues Clin Neurosci. 2003;5(1):101-8. doi:10.31887/DCNS.2003.5.1/hhippius.
- McKhann G, Drachman D, Folstein M, et al. Clinical diagnosis of Alzheimer's disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology. 1984;34(7):939-44. doi:10.1212/wnl.34.7.939.
- Roh HW, Chang YY, Kim KY, et al. Evolving Alzheimer's disease clinical practice: Updated diagnostic criteria, fluid biomarkers, and special considerations for anti-amyloid therapies. Psychiatry Investig. 2026;23(2):183-200. doi:10.30773/pi.2025.0400.
- Sperling RA, Aisen PS, Beckett LA, et al. Toward defining the preclinical stages of Alzheimer's disease: Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7(3):280-92. doi:10.1016/j.jalz.2011.03.003.
- Albert MS, DeKosky ST, Dickson D, et al. The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7(3):270-9. doi:10.1016/j.jalz.2011.03.008.
- McKhann GM, Knopman DS, Chertkow H, et al. The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7(3):263-9. doi:10.1016/j.jalz.2011.03.005.
- Jack CR Jr, Albert MS, Knopman DS, et al. Introduction to the recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement. 2011;7(3):257-62. doi:10.1016/j.jalz.2011.03.004.
- Hyman BT, Phelps CH, Beach TG, et al. National Institute on Aging-Alzheimer's Association guidelines for the neuropathologic assessment of Alzheimer's disease. Alzheimers Dement. 2012;8(1):1-13. doi:10.1016/j.jalz.2011.10.007.
- Montine TJ, Phelps CH, Beach TG, et al. National Institute on Aging-Alzheimer's Association guidelines for the neuropathologic assessment of Alzheimer's disease: A practical approach. Acta Neuropathol. 2012;123(1):1-11. doi:10.1007/s00401-011-0910-3.
- Jack CR Jr, Bennett DA, Blennow K, et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer's disease. Alzheimers Dement. 2018;14(4):535-562. doi:10.1016/j.jalz.2018.02.018.
- Jack CR Jr, Andrews JS, Beach TG, et al. Revised criteria for diagnosis and staging of Alzheimer's disease: Alzheimer's Association Workgroup. Alzheimers Dement. 2024;20(8):5143-5169. doi:10.1002/alz.13859.
- Medical Tests for Diagnosing Alzheimer's. Alzheimer’s Association. Accessed April 7, 2026. https://www.alz.org/alzheimers-dementia/diagnosis/medical_tests?.
- Alzheimer's Association workgroup publishes biology-based criteria for diagnosis and staging of Alzheimer's disease. Alzheimer’s Association. June 27, 2024. Accessed April 7, 2026. https://www.alz.org/news/2024/revised-alzheimers-diagnostic-staging-criteria.
- Dickerson BC, Atri A, Clevenger C, et al. The Alzheimer's Association clinical practice guideline for the Diagnostic Evaluation, Testing, Counseling, and Disclosure of Suspected Alzheimer's Disease and Related Disorders (DETeCD-ADRD): Executive summary of recommendations for specialty care. Alzheimers Dement. 2025;21(1):e14337. doi:10.1002/alz.14337.
- VandeVrede L, Schindler SE. Clinical use of biomarkers in the era of Alzheimer's disease treatments. Alzheimers Dement. 2025;21(1):e14201. doi:10.1002/alz.14201.
- van Dyck CH, Swanson CJ, Aisen P, et al. Lecanemab in early Alzheimer's disease. N Engl J Med. 2023;388(1):9-21. doi:10.1056/NEJMoa2212948.
- Sims JR, Zimmer JA, Evans CD, et al. Donanemab in early symptomatic Alzheimer disease: The TRAILBLAZER-ALZ 2 randomized clinical trial. JAMA. 2023;330(6):512-527. doi:10.1001/jama.2023.13239.
- Hansson O, Blennow K, Zetterberg H, Dage J. Blood biomarkers for Alzheimer's disease in clinical practice and trials. Nat Aging. 2023;3(5):506-519. doi:10.1038/s43587-023-00403-3.
- Yan JT, Dillon A, Meng T, et al. Real-world use of diagnostic tests for mild cognitive impairment, Alzheimer’s disease, and other dementias in Medicare fee-for-service beneficiaries. Alzheimers Dement (Amst). 2025;17(3):e70156. doi:10.1002/dad2.70156.
- Roth S, Yan J, Patru MM, et al. The capacity for Alzheimer's disease confirmatory testing in the United States: The current situation and simulations for future increase. J Alzheimers Dis. 2026;109(3):1458-1470. doi:10.1177/13872877251406909.
- Pahlke S, Kahale LA, Mahinrad S, et al. Blood-based biomarkers for detecting Alzheimer's disease pathology in cognitively impaired individuals within specialized care settings: A systematic review and meta-analysis. Alzheimers Dement. 2025;21(11):e70828. doi:10.1002/alz.70828.
- Schindler SE, Galasko D, Pereira AC, et al. Acceptable performance of blood biomarker tests of amyloid pathology - recommendations from the Global CEO Initiative on Alzheimer's Disease. Nat Rev Neurol. 2024;20(7):426-439. doi:10.1038/s41582-024-00977-5.
- Warmenhoven N, Salvadó G, Janelidze S, et al. A comprehensive head-to-head comparison of key plasma phosphorylated tau 217 biomarker tests. Brain. 2025;148(2):416-431. doi:10.1093/brain/awae346.
- Schindler SE, Petersen KK, Saef B, et al. Head-to-head comparison of leading blood tests for Alzheimer's disease pathology. Alzheimers Dement. 2024;20(11):8074-8096. doi:10.1002/alz.14315.
- FDA clears first blood test used in diagnosing Alzheimer’s disease. U.S. Food & Drug Administration. May 16, 2025. Accessed April 7, 2026. https://www.fda.gov/news-events/press-announcements/fda-clears-first-blood-test-used-diagnosing-alzheimers-disease.
- Alzheimer’s Association welcomes FDA clearance of first blood test for use in primary care to rule out Alzheimer’s-related amyloid pathology. Alzheimer’s Association. October 13, 2025. Accessed April 7, 2026. https://www.alz.org/news/2025/fda-clearance-blood-test-primary-care-rule-out-alzheimers-related-amyloid-pathology#.
- Mielke MM, Anderson M, Ashford JW, et al. Considerations for widespread implementation of blood-based biomarkers of Alzheimer's disease. Alzheimers Dement. 2024;20(11):8209-8215. doi:10.1002/alz.14150.
- Li Y, Lagier RJ, Racke MK, Fesko YA. Cost-effectiveness analysis of blood-based biomarker testing in the diagnosis of Alzheimer's disease pathology. J Prev Alzheimers Dis. 2026;13(3):100474. doi:10.1016/j.tjpad.2025.100474.
About the Author

Rajasri Chandra, MS, MBA
is a global marketing leader with expertise in managing upstream, downstream, strategic, tactical, traditional, and digital marketing in biotech, in vitro diagnostics, life sciences, and pharmaceutical industries. Raj is an orchestrator of go-to-market strategies driving complete product life cycle from ideation to commercialization.