The hidden liver burden in type 2 diabetes: A call to action for clinical laboratories

To take the test online go HERE. For more information, visit the Continuing Education tab.
LEARNING OBJECTIVES
1. Describe the relationship between type 2 diabetes mellitus (T2DM), metabolic syndrome, and metabolic dysfunction–associated steatotic liver disease (MASLD).
2. Identify the major clinical complications and risk factors associated with advanced liver fibrosis in patients with T2DM.
3. Compare the characteristics, advantages, and limitations of commonly used non-invasive fibrosis assessment tools, including FIB-4, ELF, VCTE, and MRE.
4. Evaluate the role of the clinical laboratory in fibrosis risk stratification, guideline-supported testing workflows, and population-based diabetes care management.
Type 2 diabetes (T2DM) is increasingly recognized as a multisystem cardiometabolic disease extending beyond glycemic dysregulation alone. Contemporary clinical guidelines now emphasize comprehensive assessment of cardiovascular, renal, and hepatic risk, creating new opportunities for the clinical laboratory to play a central role in early disease detection and risk stratification.
Among these emerging priorities, metabolic dysfunction–associated steatotic liver disease (MASLD) has become one of the most common and underrecognized comorbidities in patients with T2DM,1 with the conditions exacerbating each other.2 Driven by insulin resistance, obesity, and chronic inflammation, MASLD and T2DM share overlapping pathophysiologic mechanisms that significantly increase cardiovascular and end-organ risk.3
Reflecting this evolving understanding, clinical management has shifted from a traditional “glucose-centric” focus on HbA1c toward a broader, muti-organ approach to cardiometabolic risk management. Epidemiologic data show that more than 60% of people with T2DM have MASLD, and up to 30% progress to metabolic dysfunction-associated steatohepatitis (MASH), increasing the risk of cirrhosis, hepatocellular carcinoma (HCC), and liver-related mortality.1
An observational study employing transient elastography found that over 50% of T2DM patients had severe hepatic steatosis, while approximately 20% exhibited advanced fibrosis.4 Because fibrosis is often clinically silent, proactive identification of high-risk patients has become increasingly important.
For laboratories, this shift represents an expanded role in identifying patients at risk before irreversible liver disease develops. Historically, liver biopsy served as the primary method for fibrosis assessment. However, biopsy has recognized limitations and several validated non-invasive tests (NITs), including imaging and blood-based biomarkers, are now incorporated into clinical care pathways and guideline recommendations from organizations including the American Diabetes Association (ADA), American Association of Clinical Endocrinology (AACE), American Association for the Study of Liver Diseases (AASLD), and American Gastroenterological Association (AGA).
Metabolic syndrome and liver disease: Closing the awareness gap
Approximately 65% of patients with T2DM develop metabolic syndrome (MetS), which frequently precedes or accompanies diabetes and is characterized by central obesity, glucose intolerance, hyperinsulinemia, low high-density lipoproteins (HDLs) levels, elevated triglycerides (TGs), and hypertension. Insulin resistance is the primary driver of both MetS and T2DM.5
The combination of MetS and T2DM creates a prothrombotic (clot-prone) and pro-inflammatory state that accelerates vascular and end-organ damage, contributing to both microvascular and macrovascular complications.5,6 Key complications include the following:
- Cardiovascular disease and atherosclerosis
- Peripheral arterial disease
- Nephropathy
- Retinopathy
- Neuropathy
- Dyslipidemia
- Sleep apnea
- Polycystic ovarian syndrome (PCOS)
This metabolic environment also accelerates progression of liver disease, particularly fibrosis, which is the leading cause of liver-related morbidity and mortality.7 Because advanced fibrosis is associated with increased liver-related and cardiometabolic risk, there is growing interest in incorporating fibrosis assessment into broader chronic disease management strategies. This shift further expands the importance of scalable, laboratory-supported risk stratification approaches.
The clinical impact of underrecognized liver fibrosis in T2DM
A major challenge in managing MASLD and MASH in patients with T2DM is the silent progression of liver fibrosis. Unlike acute liver injury, fibrosis often advances without symptoms and may remain undetected until irreversible complications such as cirrhosis, portal hypertension, or HCC develop. Routine liver enzyme testing lacks sufficient sensitivity to reliably identify patients with advanced fibrosis, and normal aminotransferase levels do not exclude clinically significant disease.
Advanced liver fibrosis in patients with T2DM is associated with substantially increased all-cause mortality, driven not only by liver-related outcomes but also by cardiovascular disease and chronic kidney disease. Unlike steatosis, fibrosis severity is the strongest predictor of liver-related and all-cause mortality in MASLD with cardiovascular being the leading cause of patient death in this population.
From a health system perspective, delayed diagnosis leads to higher utilization of specialty care, emergency admissions, and transplant services. In contrast, early risk stratification enables targeted lifestyle interventions and pharmacologic therapies that may slow or even reverse disease progression. These realities have shifted the clinical focus from detection of steatosis to proactive identification of fibrosis risk, an area where laboratory-based non-invasive tests (NITs) play a pivotal role.
Guideline evolution: What’s new from ADA and AACE
Recent guideline updates increasingly recognize liver disease as a major comorbidity in T2DM. In 2025, the ADA acknowledged that liver health has been overlooked amongst those with prediabetes and T2DM despite the substantially increased prevalence of MASLD and MASH in these populations.
Similarly, the AACE 2026 guidelines for management of adults with T2DM elevate MASLD and MASH to the same level of clinical importance as chronic kidney disease and cardiovascular disease when guiding treatment decisions. This reflects a broader shift away from glucose management alone toward integrated cardiometabolic risk reduction.8
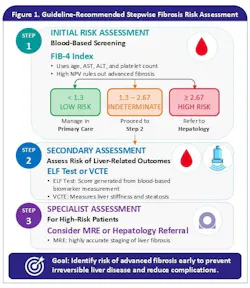
Because fibrosis is the strongest predictor of liver-related and non-liver outcomes in MASLD, both ADA and AACE now recommend structured fibrosis risk assessment using non-invasive testing. Note that AACE guidelines were written in 2022 and use the previous nomenclature of non-alcoholic fatty liver disease (NAFLD) for MASLD. Current guidance recommends initial assessment with the Fibrosis-4 (FIB-4) Index followed by secondary evaluation using the Enhanced Liver Fibrosis (ELF) test or vibration-controlled transient elastography (VCTE) in patients with indeterminate or elevated FIB-4 scores (See Figure 1).
Across professional societies, the convergence toward non-invasive, stepwise fibrosis assessment reflects a shared recognition that traditional referral-based models are insufficient to manage the scale of MASLD in patients with T2DM. Given the high prevalence of disease and limited specialist capacity, guidelines emphasize risk stratification tools that are accessible, scalable, and cost-effective. The recommended two-step approach prioritizes sensitivity to minimize missed cases while reducing unnecessary referrals.
This approach also aligns with population health strategies increasingly adopted by healthcare systems, where early identification of high-risk individuals enables focused intervention. By embedding fibrosis assessment into routine diabetes care, guidelines aim to shift liver disease management upstream, before irreversible damage occurs.
Non-invasive techniques (NITs): The laboratory perspective
Liver biopsy remains the gold standard for diagnosing MASH, but its invasive nature, cost, and associated risks limit widespread use. NITs, including blood-based biomarkers and imaging modalities are now preferred for identifying patients at low or high risk for advanced fibrosis and are increasingly replacing biopsy in routine clinical pathways.9
Active fibrosis risk stratification of liver disease in T2DM typically follows a stepwise NIT-based approach beginning with simple blood-based screening and progressing to more specialized testing for intermediate- or high-risk patients. This strategy helps identify patients at greatest risk for progression to cirrhosis and associated complications while reducing unnecessary specialty referrals and healthcare costs.10
These modalities differ in accessibility, cost, and performance, allowing their use to be tailored within stepwise clinical pathways.
FIB-4 index. The FIB-4 index is a widely used, non-invasive, and inexpensive blood-based calculation, incorporating age, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and platelet count to estimate liver fibrosis risk. Its primary strength lies in its high negative predictive value (NPV) for ruling out advanced fibrosis. Of note, it has limited accuracy in diagnosis and a high rate of false positives. Because FIB-4 uses routinely available laboratory testing data, it is especially well suited for automated calculation and large-scale population screening. However, performance of FIB-4 index can be affected by comorbidities, and it may not be accurate in patients over 65 years or in patients with diabetes.11 Patients with FIB-4 scores ≥ 1.3 are recommended for secondary assessment, while those with scores ≥ 2.67 should be considered for hepatology referral.
Enhanced liver fibrosis (ELF) test. The ELF test is a validated blood-based test granted FDA De novo marketing authorization that measures biomarkers associated with extracellular matrix remodeling and fibrosis progression, including hyaluronic acid (HA), procollagen III N-terminal peptide (PIIINP), and tissue inhibitor of metalloproteinase-1 (TIMP-1). ELF scores have demonstrated utility in assessing the risk of advanced fibrosis and provide prognostic information regarding disease progression when interpreted in conjunction with other clinical and laboratory findings. Because ELF reflects extracellular matrix remodeling and active fibrogenesis, it may provide complementary prognostic information within broader non-invasive fibrosis assessment strategies and support longitudinal risk evaluation in patients with chronic liver disease.
Vibration-controlled transient elastography (VCTE). VCTE (Fibroscan) is a non-invasive imaging technology used to measure liver stiffness and fat content (steatosis). It provides a rapid and painless alternative to liver biopsy and is widely used in MASLD assessment, although performance may be limited in patients with ascites, severe obesity, or severe narrow ribs12 (if the probe cannot reach the liver), and it can have significant intra- and inter-operator variability.
Magnetic resonance elastography (MRE). MRE is an advanced, non-invasive imaging modality that uses MRI-based technology to quantitively assess liver stiffness as a surrogate for fibrosis. It provides a highly reproducible and accurate measure of fibrosis across the full disease spectrum and has demonstrated strong diagnostic performance for detecting both significant and advanced fibrosis. Compared with ultrasound-based elastography techniques, MRE offers high diagnostic accuracy and lower operator dependence. However, its use is limited by cost, availability, and the need for specialized imaging infrastructure, which can restrict access in routine clinical practice.13
Practical considerations for clinical laboratories
Some laboratories have implemented automated fibrosis risk workflows in which FIB-4 calculations are generated directly within laboratory information systems and paired with standardized interpretive comments. In selected care models, elevated or indeterminate results may trigger reflex pathways for secondary assessment using imaging or specialized blood-based fibrosis testing, helping support more consistent risk stratification across large patient populations.
Clinical laboratories support fibrosis risk assessment through their central role in generating the test results used in initial evaluation. Routine metabolic panels already include key analytes used in calculating FIB-4, enabling laboratories to facilitate access to these assessments and support identification of patients who may benefit from further evaluation.
In clinical practice, patients with indeterminate or elevated fibrosis risk scores may undergo additional non-invasive testing to further inform risk stratification and clinical decision-making, consistent with published guideline approaches. Laboratories may support these workflows by enabling access to additional testing and by standardizing reporting formats to improve clarity and consistency of results. Such approaches can help reduce variability in ordering practices and support timely clinical evaluation. Laboratories that have adopted reflex workflows report improved identification of low-risk patients who can be safely managed in primary care, alongside more efficient triage of patients requiring specialty referral.14
Effective implementation requires collaboration with clinical stakeholders to align reporting practices, interpretative language, and integration into existing care pathways. Electronic health record integration is particularly important to ensure fibrosis risk results are clearly displayed and interpreted within the appropriate clinical context. Interpretative comments accompanying calculated scores or biomarker results may further support clinicians by providing context consistent with current clinical guidance.
From a value-based care perspective, laboratory-supported approaches to fibrosis risk assessment may contribute to more efficient patient identification and appropriate care escalation, with the goal of improving clinical outcomes through earlier evaluation. As new therapeutics for MASH become available, the demand for scalable and clinically integrated approaches to fibrosis assessment is expected to increase, further expanding the laboratory’s role in metabolic disease management.
Looking ahead, the integration of MASLD and MASH into diabetes care pathways is expected to further expand the role of the clinical laboratory in population health management and preventative care. Continued advances in laboratory diagnostics, including novel biomarkers, molecular assays, and digital risk stratification tools, are likely to further refine fibrosis assessment and disease monitoring. Ensuring standardization, appropriate test utilization, and integration into clinical workflows will be essential to realizing the full potential of these approaches in routine diabetes care.
Conclusion
Management of T2DM has evolved beyond HbA1c control toward comprehensive assessment of cardiometabolic risk, including liver disease. As recognition of MASLD and MASH continues to grow, non-invasive fibrosis assessment is becoming an increasingly important component of diabetes care pathways.
This evolution presents a significant opportunity for clinical laboratories. Through implementation of automated fibrosis scoring, coordinated use of non-invasive testing, and standardized reporting practices, laboratories can help support earlier identification of patients at risk for advanced fibrosis and facilitate timely clinical evaluation.
As clinical guidelines increasingly integrate liver fibrosis assessment into routine diabetes management, collaboration among laboratories, primary care providers, endocrinologists, and hepatology specialists will become increasingly important. Clinical laboratories are uniquely positioned to support scalable population-level fibrosis risk stratification through automated workflows, standardized reporting, and integration of non-invasive testing into routine cardiometabolic care pathways. As metabolic disease management continues to evolve toward multi-organ risk assessment, the laboratory will play an increasingly central role in early disease identification and coordinated patient care.
This article is intended solely for educational and scientific exchange purposes and is not intended as medical advice or to promote any specific product, service, or commercial activity.
References
- American Diabetes Association Professional Practice Committee for Diabetes*. Summary of revisions: Standards of care in diabetes-2026. Diabetes Care. 2026;49(1 Suppl 1):S6-S12. doi:10.2337/dc26-SREV.
- Ştefan AG, Mitrea A, Clenciu D, et al. MASH in type 2 diabetes: Pathophysiology, diagnosis, and therapeutic management-a narrative review. Medicina (Kaunas). 2026;62(2):325. doi:10.3390/medicina62020325.
- Lu X, Xie Q, Pan X, et al. Type 2 diabetes mellitus in adults: Pathogenesis, prevention and therapy. Signal Transduct Target Ther. 2024;9(1):262. doi:10.1038/s41392-024-01951-9.
- Mohiuddin MS, Neha NT, Mahir JUK, et al. Metabolic dysfunction associated fatty liver disease and type 2 diabetes: Pathophysiological links, epidemiological trends, and clinical implications. Front Endocrinol (Lausanne). 2025;16:1669478. doi:10.3389/fendo.2025.1669478.
- Asghar S, Asghar S, Shahid S, et al. Metabolic syndrome in type 2 diabetes mellitus patients: Prevalence, risk factors, and associated microvascular complications. Cureus. 2023;15(5):e39076. doi:10.7759/cureus.39076.
- Bhatt DL, Szarek M, Pitt B, et al. Sotagliflozin in patients with diabetes and chronic kidney disease. N Engl J Med. 2021;384(2):129-139. doi:10.1056/NEJMoa2030186.
- Chan WK, Chuah KH, Rajaram RB, Lim LL, Ratnasingam J, Vethakkan SR. Metabolic dysfunction-associated steatotic liver disease (MASLD): A state-of-the-art review. J Obes Metab Syndr. 2023;32(3):197-213. doi:10.7570/jomes23052.
- Samson SL, Vellanki P, Blonde L, et al. American Association of Clinical Endocrinology Consensus Statement: Algorithm for Management of Adults With Type 2 Diabetes - 2026 Update. Endocr Pract. 2026;32(4):473-518. doi:10.1016/j.eprac.2026.01.006.
- Frączek J, Sowa A, Agopsowicz P, et al. Non-invasive tests as a replacement for liver biopsy in the assessment of MASLD. Medicina (Kaunas). 2025;61(4):736. doi:10.3390/medicina61040736.
- Chen Y, Dong B, Jin X, et al. Two-step clinical care pathway to predict MASLD-related advanced fibrosis and long-term outcomes in type 2 diabetes. Gut. 2026;75(3):576-587. doi:10.1136/gutjnl-2025-337506.
- Amer J, Alnees M, Salameh M, et al. The diagnostic utility of FIB-4 as a non-invasive tool for liver fibrosis scoring among NAFLD patients: A retrospective cross-sectional study. Eur Rev Med Pharmacol Sci. 2024;28(8):3104-3111. doi:10.26355/eurrev_202404_36026.
- Shen M, Lee A, Lefkowitch JH, Worman HJ. Vibration-controlled Transient Elastography for Assessment of Liver Fibrosis at a USA Academic Medical Center. J Clin Transl Hepatol. 2022;10(2):197-206. doi:10.14218/JCTH.2021.00188.
- Imajo K, Honda Y, Kobayashi T, et al. Direct comparison of US and MR elastography for staging liver fibrosis in patients with nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol. 2022;20(4):908-917.e11. doi:10.1016/j.cgh.2020.12.016.
- Nobes J, Leith D, Handjiev S, Dillon JF, Dow E. Intelligent liver function testing (iLFT): An intelligent laboratory approach to identifying chronic liver disease. Diagnostics (Basel). 2024;14(9):960. doi10.3390/diagnostics14090960.
To take the test online go HERE. For more information, visit the Continuing Education tab.
About the Author

Anna Loh, MD
serves as a field medical liaison for hepatology with Siemens Healthineers. She is a general physician with 14 years of experience treating patients for a variety of conditions and is certified in the UK, New Zealand, and Australia.

Shalini Verma, MD, FCAP
serves as a medical officer with Siemens Healthineers. She also is a diplomate of the American Board of Pathology with active board certifications in molecular genetics pathology, hematopathology and anatomic & clinical pathology.